Do State-Level Policies Impact Maternal Mortality?
Boston College
The Issue:
Women in the United States die from pregnancy-related causes every year at a much higher rate than in most other high-income countries. But geographic location within the country impacts what conditions and policies women experience. And the mortality rate from causes related to pregnancy and childbirth varies across the different states. To what extent do state policies and programs related to women's access to family planning and reproductive health services affect maternal mortality rates?
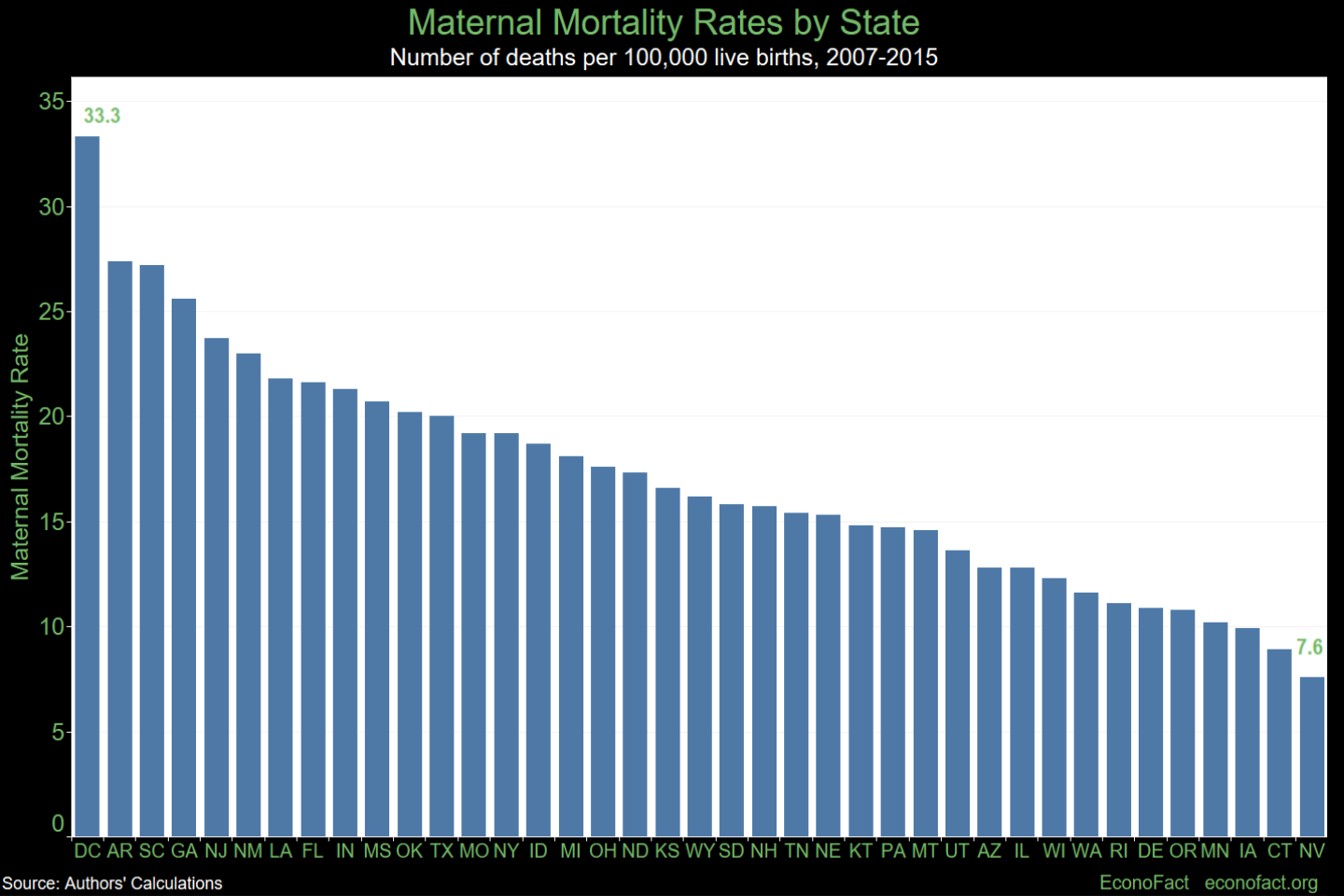
The share of women who die from pregnancy-related causes varies greatly across the states.
The Facts:
- Persistently high maternal mortality rates in the United States stand in contrast with falling global trends. The World Health Organization defines maternal death as the death of a woman while pregnant or within 42 days of the end of pregnancy from any cause related to or aggravated by the pregnancy or its management. In 2018 there were 17.4 maternal deaths for every 100,000 live births in the U.S., in total almost 700 deaths per year. As many as 60 percent of these deaths may be preventable, according to the Centers for Disease Control and Prevention (CDC). The U.S. had not published an official maternal mortality rate since 2007 because changes were made to the way in which pregnancies were recorded in death certificates and not all states implemented the change uniformly. Nonetheless, the U.S. maternal mortality rate was persistently higher than that of Canada, Japan or countries in the European Union, according to the World Bank.
- Maternal death rates in the United States differ across regions and across racial and ethnic groups. Using data from 38 states and Washington, D.C. from 2007 to 2015, we found that maternal mortality ranged from a low of 7.6 per 100,000 live births in Nevada and 8.9 per 100,000 live births in Connecticut to over 27 per 100,000 in Arkansas and South Carolina (see chart). Pregnant women in the nation’s capital were over four times more likely to die during or after childbirth than women in Nevada — with the highest rate in our study: 33.3 per 100,000. Racial/ethnic disparities are also large. African American women experience rates of mortality three times (39.9) that of white (13.8) and Hispanic (13.2) women.
- There are many possible reasons for pregnancy- related mortality. Women who are pregnant, in the act of giving birth, or within six weeks of giving birth, are at a higher risk of death if they were obese before becoming pregnant, had preexisting medical conditions, if they have a caesarean delivery or if they are older. The maternal mortality rate for women aged 35−39 years was 3 times higher than for women under 19, and for women aged 40−44 years it was 8 times higher. Pregnancy-related deaths have been associated with several contributing factors, including access to appropriate and high-quality care, missed or delayed diagnoses, and lack of knowledge among patients and providers around warning signs, according to the CDC.
- There have been many recent changes to state policies and programs related to women's access to family planning and reproductive health services, which may directly or indirectly affect pregnancy-related mortality rates. The Patient Protection and Affordable Care Act required coverage of approved contraceptive methods without co-payment. At the same time, funding cuts to Planned Parenthood have resulted in clinic closures, reducing women's access to contraception and other services. Planned Parenthood offers a range of health services for pregnant women including STD testing and treatment, birth control, well-woman exams, cancer screening and prevention, abortion, hormone therapy, infertility services, and general health care, as well as providing sex education, community outreach, and public policy work. Between 2007 and 2015 many states reduced women's access to abortion by requiring abortion providers to obtain admitting privileges at a nearby hospital; removing coverage through health insurance plans; and restricting abortions to earlier in the gestational period, in some cases to times in which some women may not be aware of a pregnancy.
- We find that Planned Parenthood clinic closures and increases in abortion limits linked to gestational age increased maternal mortality rates. Between 2007 and 2015, twelve of the states in our study enacted laws that restrict abortions based on gestational age. In the same time period, Planned Parenthood clinics closed in 27 of the states — for an average reduction of 35 percent in these states. We found that these changes were significantly related to increases in maternal mortality. We estimate that reducing the number of Planned Parenthood clinics by 20 percent increased the maternal mortality rate by 8 percent. Similarly, an additional 6 maternal deaths per 100,000 live births were attributable to the imposition of gestational age limits on abortion. The dataset we used included 4767 maternal deaths and 26,567,340 live births between 2007 and 2015 in 38 states and the District of Columbia, from the National Vital Statistics Program. We took into account racial and ethnic characteristics, as well as age. In the period of our study, five states required abortion providers to obtain admitting privileges or transfer agreements, 12 states created maternal mortality review committees, and 20 states restricted coverage of abortions by insurance purchased through the Affordable Care Act marketplace. However, we did not find differences in maternal mortality rates related to these policies or programs.
- Our analysis shows a difference across race and ethnic groups in the effect of changing laws and regulations on maternal death rates. Women in all racial and ethnic groups had higher death rates when clinics closed or gestational limits were imposed. But there were differences across these racial and ethnic groups. We estimate that a 20 percent reduction in Planned Parenthood clinics increases mortality rates 6 percent for black women, 8 percent for white women, and 15 percent for Hispanic women. In contrast, white women were the group most affected by the imposition of abortion restrictions linked to gestational age; they had a 56 percent increase in pregnancy-related death rates as compared to a 38 percent increase for all women.
What this Means:
Our research suggests that reduced access to family planning and reproductive health services through Planned Parenthood clinic closures as well as changes in laws that limit abortion by gestational age have likely contributed to higher maternal mortality rates at the state level. Since our study was conducted additional states have passed bills that reduce the gestational window of time for women to have an abortion and there are more proposed bills in the works. Our results suggest that Planned Parenthood clinic closures and laws that restrict abortions by gestational age are likely increasing the share of more risky pregnancies being carried to term. Women who carry unplanned pregnancies to term are less likely to receive prenatal care in the first trimester and their babies are more likely to be low birth weight. Greater information is needed to understand more precisely how and when state-level policies and programs impact women's decisions related to family planning and reproductive health — and how this relates to maternal mortality. Nevertheless, the available evidence suggests that reductions in healthcare access and imposition of gestational limits have serious consequences. To improve outcomes, there is a need to move beyond short-term political decisions and consider the longer-term impact on women’s health.