Could Expanding Access to Contraception Improve Economic Outcomes?
Texas A&M University and Vanderbilt University
The Issue:
Policies that gave women greater ability to control childbearing during the 1960s and 1970s have been linked to increased educational attainment, higher wages and greater labor force participation for women. This, in turn, improved their lifelong earnings and the living conditions of their children. Decades later, long-acting reversible contraceptives (LARCs) — which include intrauterine devices and subdermal implants — are showing great potential for reducing unplanned births, especially among teenagers. They are more effective than the Pill at preventing pregnancy because of their “set it and forget it” nature, but they can also be more expensive, have side effects, and require a trained provider for insertion and removal. The outlook for increasing access to these contraceptives is currently mixed. While there are several large-scale programs focusing on expanding access, a new rule from the Trump administration withholds Title X funding from clinics that offer abortion referrals and could decrease funding to LARC providers. What do we know about the short- and long-term impacts of wider access to LARCs?
Access to long-acting reversible contraceptives can have a substantial effect on teenage birth rates.
The Facts:
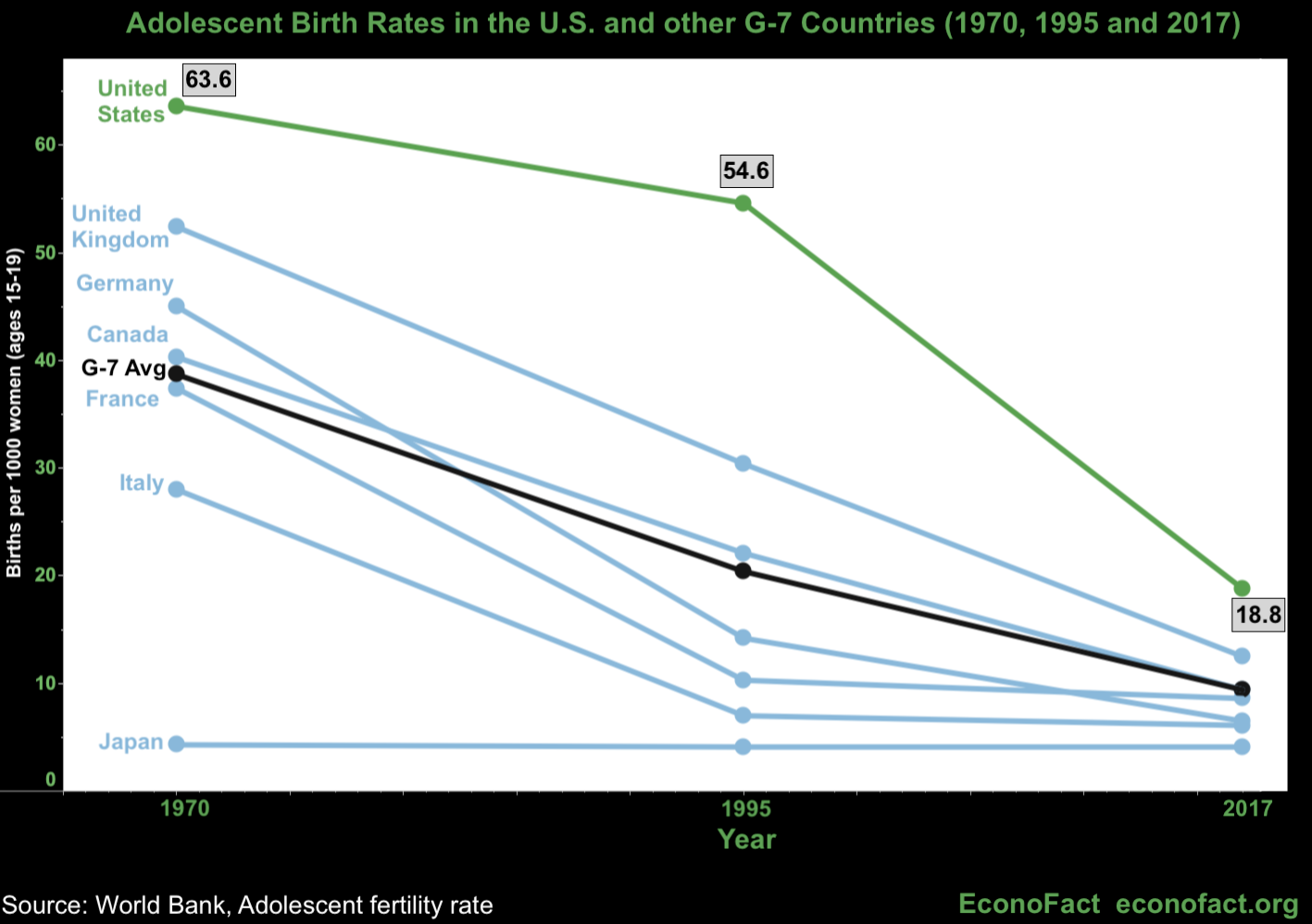
- Though the United States has one of the highest teen birth rates in the developed world, teen childbearing is on the decline. Since 2009, the birth rate for women aged 15-19 has hit a record low in each subsequent year. In 2017 the teen birth rate was 18.8 — a drop of 7 percent from 2016 (see chart below). Recent research indicates that 35% of the decline in fertility between 2007 and 2016 can be explained by declines in births that were likely unintended, and that this is driven by reductions in births to young women.
- While many factors could be contributing to the decline in teen childbearing, it is likely that long-acting reversible contraceptives are playing a role. We do not know how much of the overall decline in unintended pregnancy can be explained by greater access to and use of the most effective forms of contraception, such as long-acting reversible contraceptives (LARCs). However, it is notable that 18% of women using contraception use these methods today versus less than 5% in the late 1980s through early 2000s. LARCs include intrauterine devices (IUDs) and subdermal implants. IUDs are small, T-shaped devices that are inserted into the uterus and, depending on the product, can last between 5 and 12 years. Implants are match-sized plastic rods inserted in the upper arm, and can last up to 4 years. Since patients do not have to remember to do anything (like taking a pill or putting on a condom), LARCs are highly effective at preventing pregnancy — less than 1 in 1,000 women using LARCs become pregnant during the first year of typical use. In contrast, 9 in 100 women using oral contraceptives become pregnant, with a higher failure rate in the case of teens. Despite their high effectiveness, high upfront costs — which can go to $500 or more, with insured patients paying up to a $160 copayment — have been one of the main barriers to greater usage. It is also important to note that any woman who chooses to use a LARC also needs a trained provider for removal of the device if she wants to have children or to use a different form of contraception.
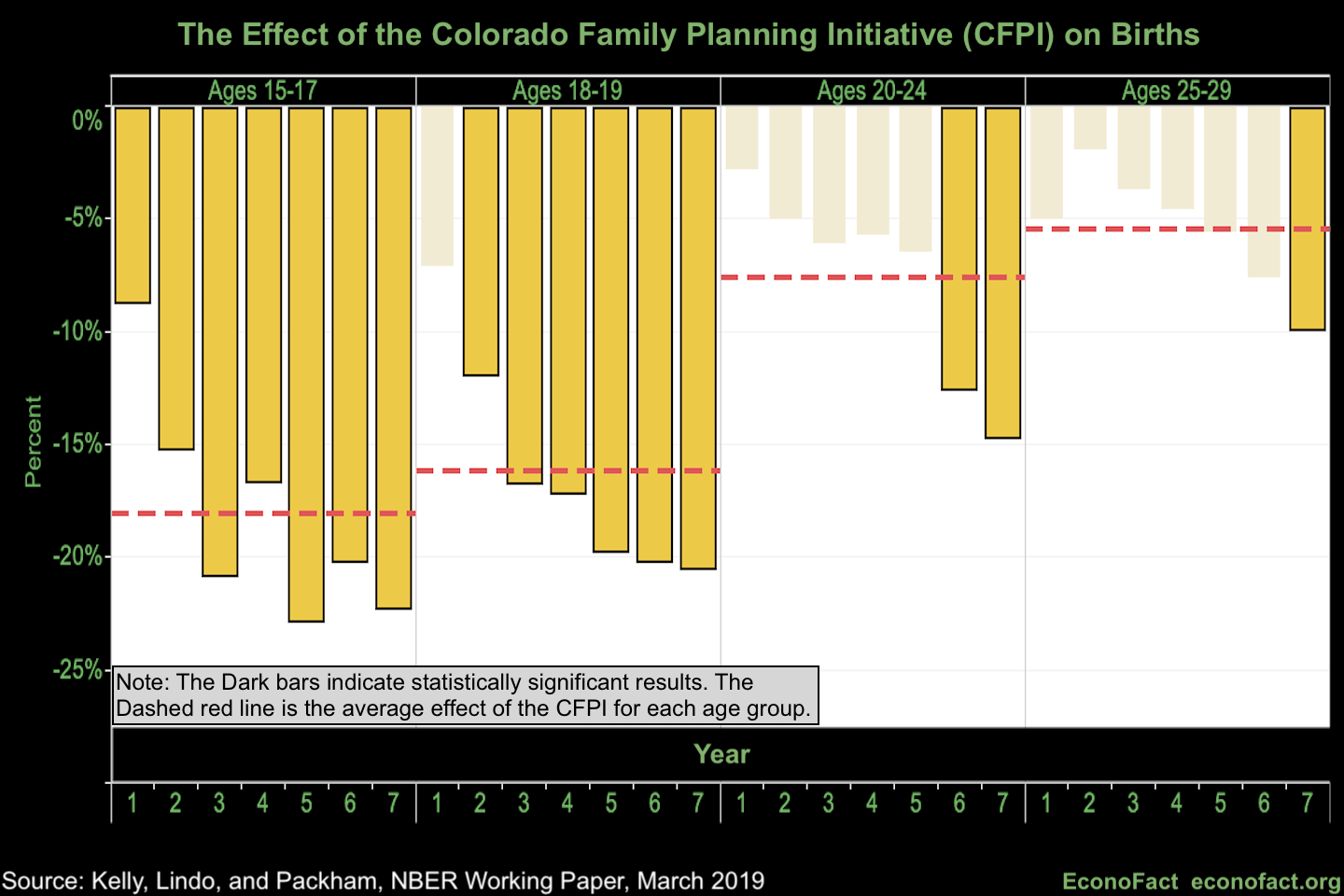
- We find evidence that expanding access to long-acting reversible contraceptives can have a substantial effect on birth rates for women aged 15-19. The Colorado Family Planning Initiative, which ran from 2009-2015, has provided researchers with the best opportunity to evaluate the causal effects of expanding access to such contraceptives because of its very large scale. This $23 million program allowed family planning clinics across Colorado to substantially expand the provision of LARCs to their low-income clients — so much so that LARC use grew from roughly 5% to 30% from 2008 to 2015 among women 15-29 years old visiting these clinics. In our research, we find that this initiative significantly reduced birth rates, by approximately 20 percent for 15-17 year olds and 18-19 year olds living within 7 miles of participating clinics. There is also evidence of effects on older women and women living farther from clinics after the initiative garnered extensive media coverage in 2014.
- Our findings suggest that the Colorado initiative also improved newborn health. We find that the initiative had effects on births that typically involve more-than-average hospital care. In particular, the CFPI reduced the number of low birthweight infants by 11.9% and very low birthweight infants by 9% born to women living near participating clinics. On the basis of this we estimate that around 480 fewer infants required extra hospital care per year in Colorado.
- Contraceptives allow women greater control of whether and when to become mothers. As a result, they improve women’s ability to invest in their education and careers, which can have a positive impact on life-long earnings. This might be particularly important in the case of teenagers, because teen childbearing is associated with lower educational attainment and increased odds of living in poverty. But the relationship between teen childbearing and poor economic outcomes is not clear-cut. Poverty is one of the factors associated with teen childbearing in the United States and it is difficult to disentangle to what extent poverty is a cause and/or a result of teen childbearing. Many of the women who become mothers in their teenage years had poor economic and educational prospects to begin with (see here).
- Past research supports the idea that reducing unintended pregnancy will improve economic outcomes, but updated research is necessary. The best evidence on the effects of unintended pregnancy on economic outcomes comes from two strands of literature. First, there are studies evaluating the consequences of unintended pregnancy shocks such as miscarriage and small differences in the timing of pregnancy. Second, there are studies evaluating changes in access to reproductive control technology during the 1960s and 1970s. Both of these strands of literature indicate that avoiding unintended births improves economic outcomes, at least to some degree (see for instance here, here and here). That said, we do not know how much these recent and ongoing efforts to improve women’s access to contraception will translate into effects on educational and economic outcomes in today's context. In order to establish the long run benefits of this kind of initiative, it is fundamental for researchers to collect and have access to relevant educational and career related data. So far, this has proven to be difficult.
- The outlook for further expansion of access to LARCS is mixed. Other major efforts to increase access to LARCs are underway. The organization Upstream has been raising funds and working with states to increase access to all forms of contraception, including LARCs. Delaware is the first state in which they have implemented their program, at a cost of $200 for every woman in the state. North Carolina, Massachusetts, and Washington have also committed to having Upstream conduct similar interventions. South Carolina has also launched a similar initiative called Choose Well with the help of the New Morning Foundation. And a smaller-scale intervention is being done in Michigan with a focus on evaluating long-term effects. At the same time, the Trump administration issued a new rule in February, 2019 that would deny federal Title X funds to any organization that refers patients for abortions. The Title X program funds reproductive health care, including services such as contraception and screenings, for about 4 million low-income people. As a result of the new rule, Planned Parenthood and other reproductive health providers announced they would leave the Title X program, which potentially means reduced access to family planning services — including LARCs — for patients.
What this Means:
Long-acting reversible contraceptives have costs and benefits. While there is evidence of their effectiveness in reducing unplanned pregnancy, there are also concerns that not all women who are given assistance with LARC insertion will have access to a provider for removal. A better understanding of the long-term effects of improved access to LARCs on women's outcomes could help inform the impact of funding decisions for such programs. The effectiveness of the Colorado Family Planning Initiative in reducing teen birth rates, together with the existing research on expanded access to contraception and improvements to women's educational and career outcomes, provide a solid basis for optimism about the potential effects of recent efforts to expand access to LARCs. However, updated research is necessary. We need rigorous and independent studies of the effects of recent and future efforts to expand access to long-acting reversible contraception. We still do not know how the Colorado Family Planning Initiative affected educational and economic outcomes. We (the authors of this Econofact article) have spent a great deal of time trying to assess the effects of this initiative on educational and economic outcomes using available survey data from The American Community Survey. Having done so, it is clear to us that surveys of the general population do not offer large enough samples for us to evaluate the effects of the initiative in a convincing manner. In the future, researchers may be able to get at this question if they are able to obtain access to larger administrative data sets, such as those from the Department of Education. Our own efforts to gain access to administrative data on educational outcomes have not been successful. It would be ideal if independent, bias-free researchers were involved in the policy design stage to ensure that it can be evaluated in a convincing manner and to ensure that appropriate program data will be collected and made available for review.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.