Impact of Medicaid Expansion on State Budgets and Mortality
University of Kansas
The Issue:
Since its implementation in 2014, the expansion of Medicaid coverage under the Affordable Care Act has been optional for states — with the federal government footing the bulk of expansion costs. As of 2021, 12 states have not expanded Medicaid and an estimated 4.0 million uninsured non-elderly adults could become eligible for Medicaid if these states opted to expand their programs. Research on the states that have expanded Medicaid is providing new evidence on the impact of expansion on state balance sheets and on population health. Recent temporary fiscal incentives included in the American Rescue Plan sweetened the deal.
Expanding Medicaid lowers mortality and does not significantly raise state expenditures. The extra federal dollars stimulate state economies.
The Facts:
- The expansion of Medicaid coverage to previously unqualified adults was a major avenue by which the 2010 Patient Protection and Affordable Care Act (ACA), also known as "Obamacare", sought to reduce the number of uninsured Americans. Health insurance coverage through Medicaid is jointly funded by a combination of federal and state funds. Prior to the ACA only pregnant women, adults with disabilities, and very low-income parents tended to qualify for Medicaid coverage. The 2010 Patient Protection and Affordable Care Act (ACA) appropriates funds for each state to expand its Medicaid program to cover all adults in families with incomes under 138% of the Federal Poverty Level, which includes low income adults that were childless and able-bodied (and therefore generally ineligible for traditional Medicaid). Rather than pay for the traditional 50-85% share of the cost that the federal government pays for traditional Medicaid (called the Federal Medical Assistance Percentages (FMAP), which vary by state), the federal agreement offered to initially pay 100% and after a few years pay 90% of the Medicaid cost for the expansion population. While the law initially made expansion a condition of not only receiving new funds but for continuing to receive existing Medicaid funds, the Supreme Court in 2012 ruled this coercive and that only the new funds could be conditional on expansion.
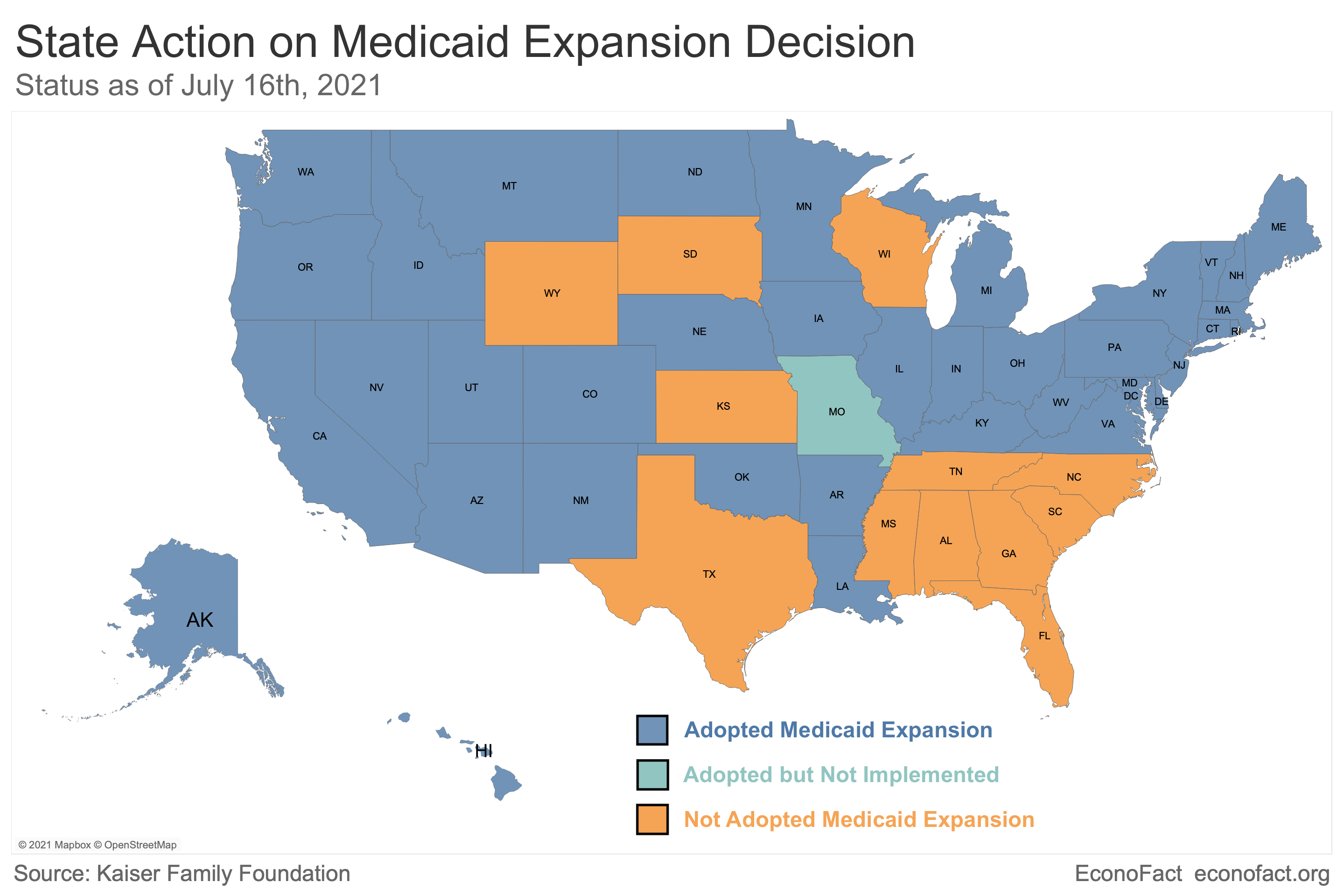
- Despite the federal government offering to cover 90% of the cost, 12 states (Alabama, Florida, Georgia, Kansas, Mississippi, North Carolina, South Carolina, South Dakota, Tennessee, Texas, Wisconsin, and Wyoming) had still not expanded Medicaid by the end of the Trump administration. In order to encourage additional expansions, the Biden administration included a provision in the March 2021 American Rescue Plan offering to increase the FMAP for traditional Medicaid by 5 percentage points for a period of two years to any holdout state that expanded Medicaid per the ACA. In all cases those new additional funds for traditional Medicaid would be larger than the state’s share of the cost of the Medicaid expansion. For example, if Kansas were to adopt Medicaid expansion and all the newly eligible adults were to enroll, the state 10% share of expansion coverage would be $210 million in FY 2022-2023, according to estimates from the Kaiser Family Foundation. But, the state would also stand to receive an estimated additional $450 million in federal dollars from the 5% additional contribution to the FMAP for traditional Medicaid enrollees. (After two years, new expansion states would continue to receive the 90% match for the expansion group and the traditional match without the 5 percentage-point increase for the traditional population.)
- Research on states that already expanded Medicaid finds no clear change in overall spending from state funds, despite states having to pay for at least 10% of the expansion. A study that analyzed budget data from all 50 states from 2010-2018 comparing changes in each category of spending between Medicaid expansion states vs. non-expansion states found that Medicaid expansion increased total spending in expansion states by 6% to 9%, compared to non-expansion states. Not surprisingly, expansion states experienced a substantial increase in Medicaid spending. Importantly, however, the study found that this increase was subsidized entirely by increased federal funding to expansion states. Medicaid expansion resulted in a 12-24% increase in state spending from federal funds, relative to states that didn’t expand. This is as to be expected, given that the federal government paid for at least 90% of the expansion. In contrast, there is no clear evidence that spending from state funds increased to the same degree. The authors of the study found that changes in spending from state funding were modest and not statistically significant, with less than a 1% increase from baseline for 2017 and 2018. There is also no evidence that states made up for the funds required to cover their share of expansion by making cuts in other areas, with researchers finding no clear increase or decrease in individual categories of state spending. This is true regardless of what area they looked at, such as K-12 education, higher education, transportation, or corrections.
- What explains the absence of significant increases in state expenditures in expansion states? In part, it is likely that the Medicaid expansion helped to offset other prior state expenditures for health care services that states were providing on their own through public clinics, mental health facilities and public hospitals, among others. But the expansion also had other fiscal effects on states. A case study from Michigan provides an illustration of how some states were even expected to net revenue increases from Medicaid expansion. The authors estimate that for the 2021 fiscal year, the state would spend $399 million for Michigan’s 10% of expansion costs, but save $235 million in spending on programs for community mental health, adult benefits waiver, and corrections health care, and take in an additional $178 million from taxes on hospitals and long-term care. The expansion would also have positive economic effects on population growth and tax revenue. All of this together would yield a $43 million increase in net revenue.
- All of the additional federal spending also has a positive economic multiplier for states. We can use past expansions of federal spending to quantify this effect. The 2009 American Recovery and Reinvestment Act, allocated $800 billion in new federal spending using existing funding formulas that may not have been correlated with that recession, which would allow the quantification of a causal effect. (If spending had been allocated depending on the severity of the local recession, then it would be difficult to isolate the impact of the federal stimulus from the fact that the most impacted states had greater economic room for recovery.) The best estimate of the multiplier of federal spending for the gross state product at 1.53. This means that — as a result of the increases in employment, income and consumption that it brings to the state — every additional federal dollar spent increases state economic output by an estimated $1.53. Similarly, the estimates based on the aftermath of the Great Recession found a multiplier for job-years per $100K spent to be 2.01 (so each $49,750 spent created one job for one year) during that period.
- New evidence finds that states that expanded Medicaid experienced a drop in mortality of the target population. A recent study that combined survey and social security mortality data finds that prior to the ACA expansions mortality rates across expansion and non-expansion states trended similarly. However, beginning in the first year of the policy, there were significant reductions in mortality in states that opted to expand Medicaid relative to states that did not. Those ages 55–64 with either less than a high school degree or income under the threshold (138% of the Federal Poverty Level) in expansion states experienced a 9.4% drop in mortality after expansion, compared to non-expansion states. A separate study with a mostly different methodology confirms the finding of reduced mortality after expansion. The 9.4% drop corresponds to substantial excess deaths per year in non-expansion states. Scaled by the sample population, annual excess deaths range from 16 in Wyoming and 21 in South Dakota to 72 in Kansas and 135 in Mississippi to 694 in Florida and 730 in Texas.
What this Means:
States not expanding Medicaid is resulting in excess deaths among inhabitants of the state. By most calculations of the value of a statistical life, preventing these deaths alone justifies an expansion of a government program for which the state only bears 10% of the cost (e.g., in Kansas, saving 72 lives at a cost of $210 million or $2.9 million per life, which is far below the current EPA estimate of $9.8 million). And this is only the mortality benefits of expansion, and so does not include many other documented benefits, including very recent work showing a 34 percentage point relative decline in new medical debt in states that expanded in 2014. Moreover, states may not end up even paying all of that 10% in net, given offsets from other existing programs and increased provider tax revenue. Even beyond that, to incentivize expansion, the Biden administration will also increase traditional Medicaid funding in a state at a greater magnitude than the 10% cost to a state. So even with the most conservative dynamic assumptions Medicaid expansion saves the state both lives and dollars. And these federal dollars also help the state economy and create new jobs. Given all of these reasons the remaining holdout states have few if any defensible economic or public health reasons to refuse to expand Medicaid.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.