Containing Prescription Costs in Medicare
Northwestern University
The Issue:
Pharmaceutical pricing in the United States is a complicated and opaque process. Concern about the high and rising prices of prescription drugs has led to legislative and policy activity, including provisions passed as part of the 2022 Inflation Reduction Act (IRA). This monumental legislation allowed Medicare to “negotiate” certain drug prices for the first time and changed the cost-sharing structure of its prescription drug benefit. This new law represents the first attempt at giving government officials the power to effectively set the prices of prescription drugs in the United States and should help lower both consumer out-of pocket expenses and the burden on Medicare spending. However, it may also have adverse implications for firms’ incentives to invest in innovative new drugs in the future.
Medicare will now have a more direct role in setting prices for certain drugs. This should help address high and rising prices of some prescription drugs. But it could also negatively affect firms' incentives to invest in new drug development.
The Facts:
- Medicare is the country’s primary public health insurance program, providing coverage for elderly and disabled Americans. The program’s retail prescription drug benefit, known as Medicare Part D, covered about 50 million beneficiaries in 2022 and accounted for 30% of total US prescription drug spending in 2017. Part D coverage is administered by private health insurers (known as plan sponsors), such as UnitedHealth or CVS Health. These plan sponsors negotiate prices with drug manufacturers and contract with pharmacies to dispense drugs to plan enrollees, who are able to choose among a selection of Part D plans with different premiums and deductibles.
- Historically, Medicare (or, more precisely the Center for Medicare and Medicaid Services, CMS) has been barred from directly negotiating the price of drugs in Part D with manufacturers. This provision was intended to promote market competition and limit the federal role in the program. While private firms strenuosly negotiate with pharmaceutical manufacturers over prices, their bargaining power is limited by the need to provide consumers with insurance products that provide access to the pharmaceutical products they demand. Some were concerned that Part D expenditures were projected to comprise an increasing share of overall Medicare spending.
- Another concerning feature of Medicare Part D was its cost-sharing structure. Under the system pre-IRA, Medicare patients could face very large out-of-pocket payments for expensive drugs. A number of patients without supplemental insurance coverage face uncapped liabilities when they required expensive medications.
- As part of the IRA, Medicare will now have a more direct hand in setting prices for the drugs that account for the most spending in the Medicare program. Under the IRA, the CMS has authority to negotiate prices for high-cost drugs. Drug manufacturers unwilling to accept the price negotiated by CMS will either be forced to stop selling all their products to the Medicare system or pay fines that could amount to more than the drug’s overall revenue. This means that CMS will effectively have an unfettered ability to set prices for certain drugs.
- The CMS recently announced the first 10 drugs eligible for negotiation. These ten drugs accounted for the highest total gross Part D covered prescription drug costs, among those that met several criteria (such as not having generic competitors and having been on the market above a set amount of time). The ten drugs selected include blood thinners along with drugs treating diabetes and autoimmune disorders, and accounted for 20% of gross Part D prescription drug costs from June 2022 to May 2023. To be eligible, drugs needed to have been on the market for at least 9 years by 2026 (in the case of small-molecule products, generally meaning those taken orally and sold at pharmacies) or 13 years for large-molecule drugs (i.e. those generally injected and taken with medical supervision). The products must also not face competition from a generic or biosimilar susbtitute. The prices negotiated for these first drugs will be applicable starting in 2026, with 50 more drugs subject to negotiation by 2029.
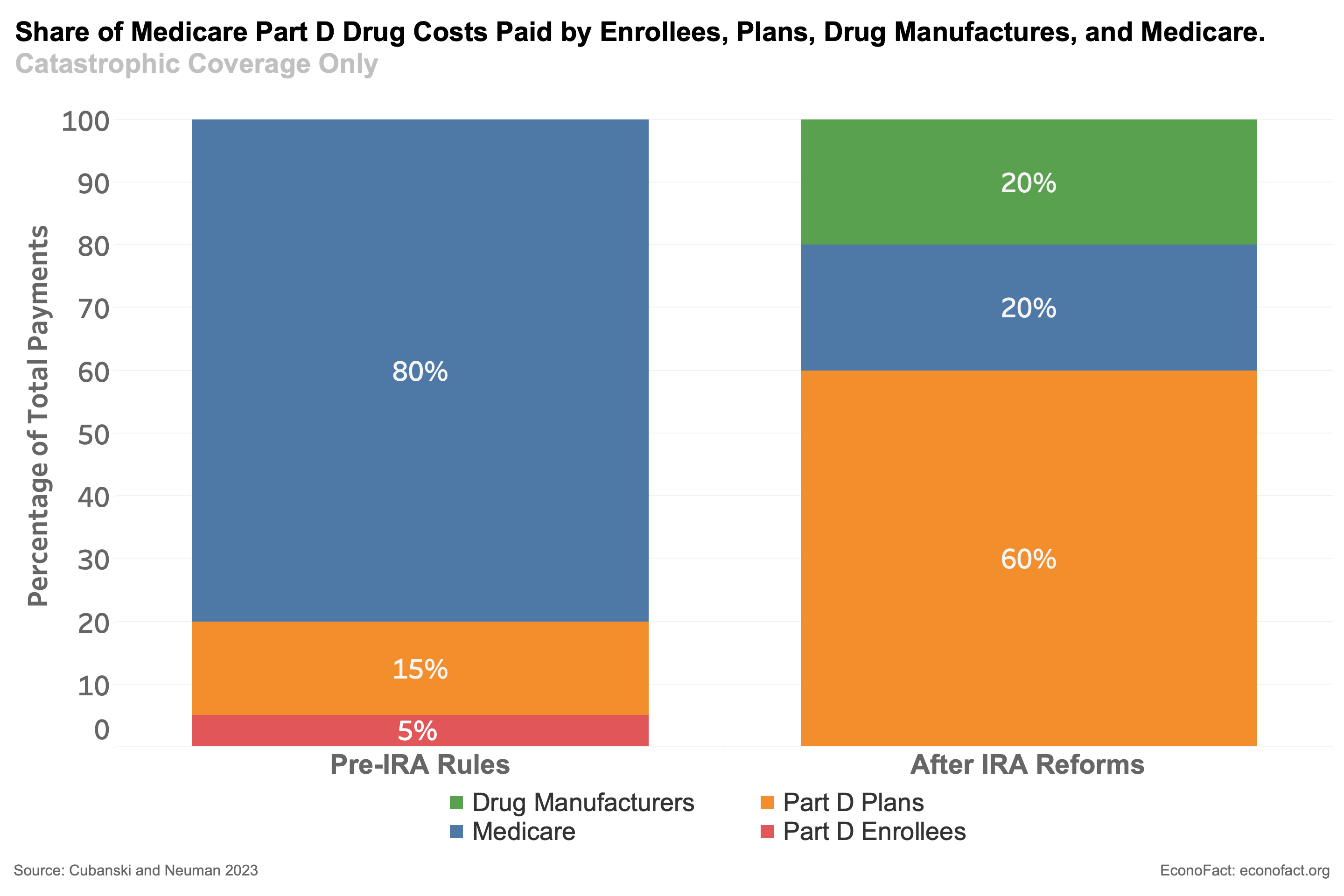
- The IRA also addressed the high cost-sharing provisions that are a current feature of Part D plans. In general, Part D costs are split between enrollees, Part D plan sponsors, drug manufacturers, and the government. Under pre-IRA allocation rules, patients who use expensive pharmaceuticals face high exposure to the cost of their drugs. For example, patients taking certain cancer drugs (such as Revlimid and Pomalyst) could face an annual drug cost upwards of $8,000 or even $10,000. However, for individuals who have not secured supplemental insurance coverage, there is no upper limit on their expenditures. Many patients with conditions such as cancer, autoimmune diseases, asthma, and HIV spend thousands of dollars out of pocket each year. The situation is different under the pre-IRA situation when Medicare Part D enrollees enter the “catastrophic phase” of their coverage, which occurs after paying $7,400 in out-of-pocket spending. The contribution of the enrollee falls to only 5% of remaining costs, as shown in the column of the figure labeled “Pre-IRA Rules”, while the government is responsible for 80% of the costs and Part D plan sponsors pick up the remaining 15%. But, as discussed below, the IRA will change this allocation.
- The current cost-sharing structure for Part D may encourage higher drug prices as well as containing the expenditures of both plan sponsors and drug manufacturer at the expense of both enrollees and the taxpayers. Research finds that a drug with a higher fraction of people taking it who are on Medicare experienced faster growth in the product’s list price. This finding indicates that drug manufacturers and Part D plan sponsors are responding to financial incentives – namely, the large shares of costs covered by both patients and the government – to raise the list price of certain drugs, although doing so increases the burden on patients and the Medicare budget.
- The IRA will meaningfully change the shares of Part D drug spending to be borne by consumers, plan sponsors, drug manufacturers, and the government. The figure illustrates the change from the current situation to the one when the IRA is in force in 2025. The largest change once the IRA reforms are fully phased in will be to eliminate any enrollee responsibility for spending in the catastrophic phase. The government's share of spending in this period will be reduced to 20%, while Part D plan sponsors will be now responsible for 60%. The IRA reforms also include a cap on total annual patient out-of-pocket expenditures of $2,000. However, there are still several drugs that would automatically put patients at this limit each year simply as a result of their chronic—and known—condition.
What this Means:
These two provisions of the IRA should provide meaningful steps to address high and rising prices of prescription drugs, but do so in quite a blunt way that could negatively affect incentives to invest in future drugs. It should be recognized that actions to reduce drug prices almost always involve a tradeoff between lower costs today against more limited access and reduced incentives to develop better drugs for the future. This includes both the initial decision to develop the drug and decisions about launching and funding trials to find additoinal uses for existing drugs. This cost is particularly high for the growing segment of specialty products known as biologics, which often are able to treat a number of unrelated conditions. While this tradeoff is one that policymakers must carefully consider upfront when reforming the drug pricing system, there is little evidence that occurred in the crafting of the IRA. This tradeoff is particularly relevant to the government’s attempt at drug price negotiation in Part D. Such price setting power could have meaningful implications on the investment decisions of firms, since these changes could reduce the expected returns for companies developing new drugs, lowering their incentives to invest new funds in research and development of tomorrow's drugs.
Topics:
Public HealthLike what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.