COVID-19 and Medicaid: Can State Budgets Handle It?
Emory University, Rollins School of Public Health and Urban Institute
The Issue:
Recessions in the U.S. mean not only loss of jobs but also loss of employer-sponsored health insurance. This is especially problematic during the coronavirus pandemic, which poses a simultaneous public health crisis and a national economic downturn. The Medicaid program, which covered nearly 69 million Americans as of July 2020, is uniquely situated to support both health insurance coverage and economic recovery. Its enrollment increases during economic downturns, even while states’ revenues decline, and the automatic transfer of federal funds to states administering the program serves as an economic stabilizer — increasing public spending when other forms of spending are in retreat. However, the ability for Medicaid to serve these two important roles depends on states' ability to fund their share of the program.
During recessions, Medicaid can play a key role in supporting health insurance coverage and economic recovery. But, its ability to do so depends on states' ability to fund their share of the program.
The Facts:
- Medicaid provides health coverage to low-income and disabled Americans and its role has expanded since the passage of the Affordable Care Act. The COVID-19 economic downturn is the first since the Affordable Care Act (ACA) increased the role of Medicaid in covering low-income adults in the 37 states that have implemented ACA Medicaid expansion. Historically, Medicaid eligibility was limited to low-income individuals of particular groups (children, pregnant women, parents of dependent children, elderly adults) and individuals with disabilities. The Affordable Care Act gave states the option to expand Medicaid to cover nonelderly adults with income up to 133% of federal poverty, with the federal government now providing 90% of the funds. While almost half of Americans receive health insurance coverage through their jobs, Medicaid, is the second-largest source of health insurance, covering about one-fifth of the population in 2019.
- The COVID-19 pandemic led to high rates of employment loss putting workers' access to employment-sponsored health insurance at risk and leading to increases in Medicaid enrollment. Unemployment spiked between March and April of 2020 when the unemployment rate peaked at 14.7% with about 23 million Americans classified as unemployed. Although the labor market showed steady improvement, more than 10 million Americans were still unemployed as of November 2020 (almost twice as many as in November of 2019), according to Bureau of Labor Statistics. Service industries, which are highly represented by low-income and minority workers, were most affected. Workers in retail, health care, and service industries represent nearly half of low-wage workers across states and are likely to either already be Medicaid eligible or to become eligible after a loss of paid employment. Among families experiencing job loss, some may remain eligible for employer-sponsored health insurance through another working family member. But, estimates suggest that between 2 and 7.3 million fewer people will receive health coverage through their employer as a result of the downturn. An estimated 4.3 million people will gain coverage through Medicaid/CHIP and 400,000 more people will gain Marketplace coverage, while 2.9 million people will become uninsured. In 28 states reporting early impacts, Medicaid enrollments barely grew from January to March but grew by 3% to 10% from January to May as the economy shrank.
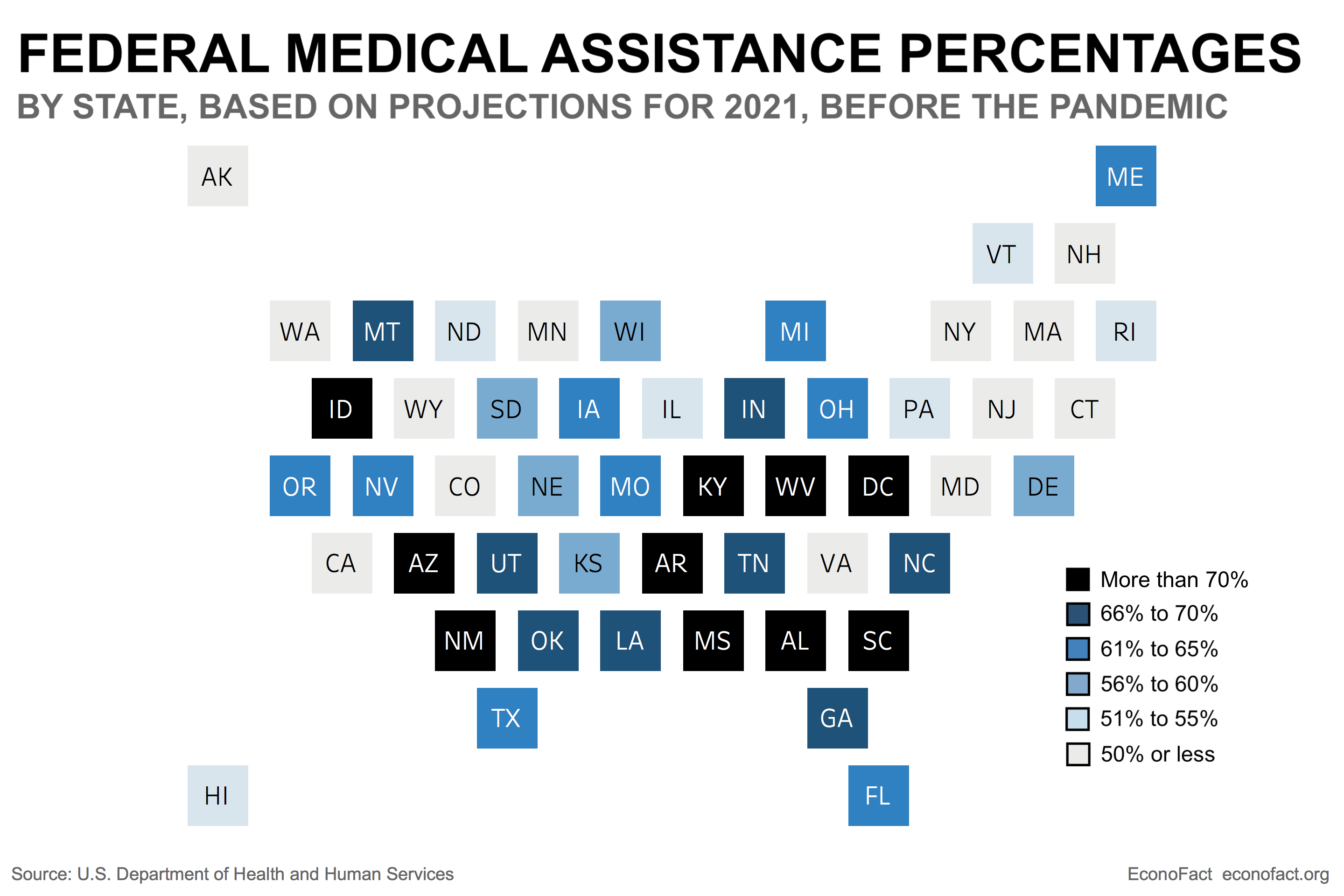
- The counter-cyclical nature of the Medicaid program has served as an automatic stabilizer in the past. In prior recessions (before the ACA's Medicaid expansion), every percentage point increase in the unemployment rate roughly translated to an increase in Medicaid enrollment of about 1 million new enrollees. Shared federal/state financing serves as an "automatic stabilizer" by providing states an average matching percentage of 60.4% for each dollar of spending on traditional Medicaid enrollees. The Federal Medical Assistance Percentage (FMAP) is set inverse to states’ per capita income, ranging from 50% for 13 states to 77% in Mississippi (see chart). During prior recessions, there have been temporary increases to the FMAP. In addition, the federal government provides a 90% match for spending on the ACA expansion group. The federal dollars stimulate state economies as the dollars flow through the health care and other sectors. Yet, states have to come up with their share of Medicaid spending using state tax revenues.
- Congress passed two major bills addressing COVID-19 with implications for state budgets and the Medicaid program—the Families First Coronavirus Response Act (FFCRA) and the Coronavirus Aid, Relief, and Economic Security (CARES) Act. The FFCRA, amended by the CARES Act, increased the FMAP by 6.2 percentage points but also required states to maintain eligibility rules and premiums as of January 2020, cover COVID-19 testing and treatment, and provide continuous eligibility for all individuals enrolled in Medicaid as of March 2020 through the end of the public health emergency. This maintenance of effort (MOE) requirement increases Medicaid costs for states covering individuals who would otherwise have lost Medicaid due to changes in income or other eligibility pathways (e.g., pregnancy) for an unknown duration (as long as the COVID-19 crisis continues). The current increase in FMAP is the same as under the American Recovery and Reinvestment Act (ARRA), but does not include the ARRA’s additional increase for states with higher than average unemployment rates — which directed more aid to states whose budgets suffered greater shortfalls due to relatively worse employment impacts from the crisis.
- States are anticipating revenue shortfalls for their fiscal year 2021 budgets as well as increased spending due to Medicaid enrollment growth and other coronavirus-related outlays. While administrative data on Medicaid enrollment lags, increases are projected to be much larger in states that have expanded Medicaid under the ACA (7.3% increase covering 3.7 million people) than in states without Medicaid expansion (3.1% increase, 600,000 people). States anticipate increased Medicaid enrollment and spending of 8% in 2021 due to a continued recession but also due to the Maintenance of Effort (MOE) under the Families First Coronavirus Response Act (FFCRA). Since most states rely heavily on general and selective sales taxes, their budgets are directly affected by a slump in consumer spending. Compared with a year prior, the average state GDP fell 9% by the second quarter of 2020. The fiscal stimulus provided by the federal government buffered the effects on consumer spending through the second quarter of 2020, but the lack of additional stimulus is likely to result in a slower economy through the end of the year. Losses in state tax revenues and increased spending could result in budget shortfalls as great as $125 billion in total for all states in 2021 with wide variation across the states, according to one estimate.
- States’ abilities to balance their budgets while maintaining their current levels of Medicaid spending remains uncertain. States are required to balance their budgets, do not have fiscal tools to finance deficits as the federal government does, and strong anti-deficit provisions have been found to reduce state spending by $44 for every $100 deficit overrun. When states are forced to find large budget cuts, Medicaid programs are often the target — more than half of states cut Medicaid payments to providers during the Great Recession, and some states have already cut Medicaid programs in 2020.
- The federal government could implement additional policies to provide fiscal relief for states. Given the unanticipated and extraordinary impact of COVID-19 on states’ budgets, the federal government could mimic the earlier ARRA provisions to recognize differences in states’ unemployment rates. If made permanent, this type of adjustment would enhance the automatic counter-cyclical effect of the Medicaid grant, as recommended by the U.S. Government Accountability Office.
What this Means:
The counter-cyclical nature of the Medicaid matching grant is a critical asset to states as COVID-19 imposes great uncertainty surrounding increased enrollments, state spending and budget shortfalls. The benefit of this federal transfer of resources to states could be strengthened if the increased FMAP now in place was adjusted upward specific to states’ relative level of unemployment and phased out as the public health emergency and MOE for Medicaid ends, much like the adjustment implemented in response to the Great Recession. Given states’ inevitable budget short falls in fiscal year 2021, direct federal stimulus to state/local governments is needed. Without this, the economic downturn related to Covid-19 will worsen as state/local government workers become unemployed and another round of losses in health insurance threaten families and states’ budgets.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.