How Opioid Overdoses Reached Crisis Levels
Northeastern University
The Issue:
More than 90,000 people died of a drug overdose in the U.S. during 2020 — a 30 percent increase over the prior year — and the 12-month death toll hit over 100,000 deaths if you focus on the first 12 months of the pandemic, between April 2020 and April 2021. Drug overdose deaths had been on the rise for two decades in the United States before the pandemic spike. But the problem has been evolving in nature. The opioid crisis started with over-prescribing of prescription painkillers and has since shifted to more dangerous and illegal substances including heroin and fentanyl. Recent restrictions on prescribing and greater use of prescription drug monitoring programs have sought to reduce the supply of opioids while increased funding for substance abuse treatment has focused on decreasing demand. Although neither approach has been proven effective on its own, a multipronged approach appears to offer the most hope.
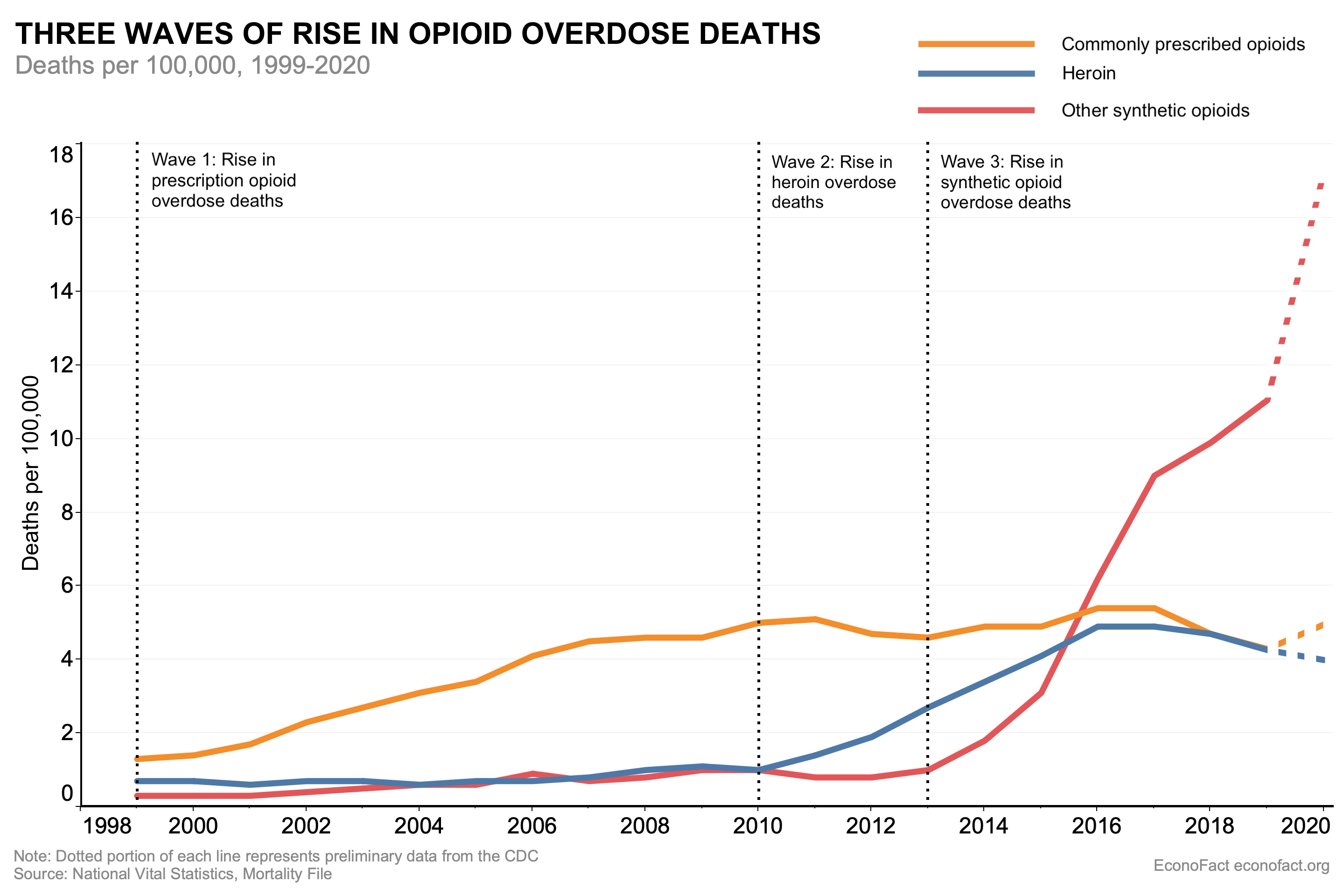
The rise in opioid overdose deaths began with prescription painkillers, with subsequent increases fueled by heroin and fentanyl.
The Facts:
- Increasing drug overdose deaths in the United States have largely been driven by opioids. During 2019, before the onset of the pandemic, 70,630 individuals died from a drug overdose — six times greater than the number in 1999, with opioids involved in 70% of the deaths. The annual death toll from opioids was higher than the number of Americans killed by HIV AIDS or guns in any single year. Drug overdose rates have been higher and rising more rapidly among men over the past two decades and more recently among those aged 25 to 34 years. With the onset of the COVID pandemic, the combination of increased stress, reduced access to care, and greater prevalence of more lethal drugs led to a record number of 93,000 drug deaths in 2020 with roughly 69,000 from opioids. Although opioid overdose-related death rates among non-Hispanic whites have typically exceeded that of other groups, rates among Blacks have risen more steeply in recent years, a trend that preliminary data indicates may have accelerated during the pandemic. And monthly state data indicates that overdose rates remained elevated in 2021.
- The rise in opioid overdose deaths occurred in three distinct waves arising initially from prescription opioids such as OxyContin, then switching to illegal opioids such as heroin, and finally moving to synthetic opioids — primarily fentanyl. The first wave began in the 1990s with increased prescribing of opioids, such as OxyContin for the medical management of pain. The most commonly misused prescription opioids were Hydrocodone (such as Vicodin®), Oxycodone (such as OxyContin®), and Codeine. Since 2010, the death rate from prescription opioids leveled off at around 5 deaths per 100,000 (see chart). The slowdown in the mortality rate coincided with decreases in the amount of opioids prescribed in the U.S., attributed to both growing awareness of the risks associated with prescription opioids as well as to state-level policies aimed to reduce over-prescribing. Yet as prescription opioid deaths plateaued, a second wave of the opioid crisis began in 2010 with rapid increases in overdose deaths involving heroin. There is evidence of substantial connection between prescription opioid abuse and heroin use. In a sample of heroin users in a treatment program, 75% of those who began opioid abuse after 2000 reported that their first regular opioid was a prescription drug and that heroin often is more readily accessible, less expensive, and offers a more potent high than prescription opioids. As of 2016, the death rate for heroin also began to level off at around 5 deaths per 100,000. However, even before the rate of heroin deaths slowed, a third wave began in 2013, with significant increases in overdose deaths involving synthetic opioids – particularly illicitly manufactured fentanyl, which is 50 to 100 times more potent than morphine. Illicit fentanyl can be found in combination with heroin, counterfeit pills, and cocaine—making it much more lethal as it is difficult for users to determine the dosage. As of 2019, the death rate due to illicit fentanyl was 11.4 per 100,000 and still rising.
- One response to the growing addiction crisis has centered on efforts to restrict the supply of prescription opioids. Many states have passed laws limiting opioid prescribing for acute pain in first-time opioid users to a 7-day supply or shorter (see here). However, the effectiveness of these restrictions on reducing the risk of opioid dependence or mortality is unclear. The Centers for Disease Control and Prevention warns that the risk of long-term opioid use increases with each additional day of taking the pills — starting with the third day. Another strategy aiming to reduce the abuse of prescription opioids relies on Prescription Drug Monitoring Programs, which make it more difficult for people to receive prescription opioids from a physician by allowing physicians to view the prescribing history of a given patient. These programs are intended to limit “doctor shopping,” or the practice of visiting several doctors in order to receive a high quantity of prescription opioids. There is recent evidence that monitoring programs that require physicians to check the database on all cases — not just those that are suspicious — reduce indicators of opioid abuse. However, restrictions on prescribing that make it more difficult for people to access opioids from legal channels might have unintended consequences if, for example, it induces people to seek illicit opioids on the black market, which often increases the likelihood of an overdose.
- The number of opioid prescriptions in the U.S. has declined markedly. However, the dispensing rate varies greatly by location and by provider and remains very high in areas of the country. The overall opioid-prescribing rate in the United States has declined from a peak of about 81 opioid prescriptions written for every 100 Americans in 2012 to about 43 per 100 in 2020 (see here). But prescription rates vary greatly. Prescribing of opioids per capita is significantly higher in rural versus urban counties and in places that experience higher rates of “deaths of despair”— deaths related to opioid overdose, alcohol abuse, and suicide — as well as higher rates of unemployment and lower rate of insurance coverage. In addition, prescribing rates are higher where there are more dentists and primary care physicians per capita. And, research shows that emergency room patients treated by physicians who prescribe opioids more often are at greater risk for long-term opioid use even after a single prescription than those who see less-frequent prescribers.
- With continued over-prescribing, the likelihood that opioid medications are diverted from the primary patient to secondary users is quite high. The 2018 National Survey on Drug Use and Health found that more than half (51.3 percent) of people who misused pain relievers in the past year obtained the last pain reliever from a friend or relative. Preliminary findings from a Massachusetts pilot program that encourages patients to return unused opioid prescription medication indicate that patients who return unused medication typically return at least half of the pills that they had been prescribed. This finding suggests that physicians may still be prescribing more medication than is necessary even when an opioid is warranted.
- Policy responses on the demand side largely include various types of addiction treatment, including the use of medication-assisted therapies. Access to substance abuse treatment in the U.S. has been limited and many counties with relatively high drug-induced death rates do not have a single stand-alone substance use treatment facility. Medication-assisted therapies involve drugs that can satisfy opioid dependence without producing the same euphoric effect as heroin, such as methadone and buprenorphine. Evidence suggests that increased access to these treatment opioids is associated with decreased overdose deaths. One Massachusetts study found that treating opioid overdose survivors with buprenorphine or methadone was linked to a 40% to 60% drop in mortality 1 year later (see here). Yet, sufficient adherence to these medication-assisted therapies is often very low. For example, the minimum recommended duration for buprenorphine/naloxone treatment (also known as Suboxone) is one year or more. Yet studies indicate that 25 to 30 percent of patients discontinue treatment within the first month and 50 percent or more of patients discontinue within 6 months. Moreover, the number of providers that can prescribe these medications is restricted. However, new federal guidelines released in April 2021 will reduce regulatory hurdles to allow far more medical practitioners — such as nurse practitioners and physician assistants — to prescribe buprenorphine in treating opioid use disorder, potentially increasing access particularly in rural areas where there are few physician prescribers. And Medicaid expansions have improved coverage and medication-assisted therapy access for substance-abuse patients.
What this Means:
The economic burden of opioid abuse is vast, including healthcare costs, addiction treatment, lost productivity, and policing and imprisonment. This is on top of the incalculable costs from the loss of life and broken families that are associated with the opioid abuse crisis. Yet there is no silver bullet that can fix the current situation. Efforts to rein in the supply of prescription opioids often have unintended consequences such as driving current users to seek out more dangerous drugs such as heroin and fentanyl. Efforts to reduce demand through addiction treatment are costly and prolonged. Like most complex social problems, the solution to the opioid crisis has to be a multipronged approach. We need to simultaneously pursue preventive measures that decrease the initial prescribing of opioids in favor of alternatives to pain management while maintaining their use for those with chronic pain. These approaches need to be balanced with ensuring that patients suffering from opioid use disorder have access to the most effective forms of treatment as well as harm reduction methods such as safe/supervised injection sites and naloxone to prevent as many overdose deaths as possible. Without continued and coordinated action, we risk reducing access to substance-use treatment just as our opioid-related care needs are at their peak.
Topics:
Public HealthLike what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.