Lives vs. Livelihoods? Lessons from the Ebola Epidemic
Swarthmore College

The Issue:
Save lives or save livelihoods? Social distancing measures can take a heavy economic toll, by interrupting normal economic activity and imposing a short-run tradeoff between improving the health of the population and hurting the economy. Over time, this tradeoff can be defeated by intervening aggressively and persistently enough to scale back the overall size of the epidemic. At each point along the way, however, policies that make it safer for people to interact are an essential complement to policies that tell people to interact less. In the short run, adaptations that make interacting safer allow vital components of the economy to continue to function. Once the outbreak is under control, they play a crucial role in getting people back to work safely. The West African Ebola crisis that began in late 2013 offers insights that are valuable for the current novel coronavirus pandemic about the importance of early action and preparedness and about the difficult tradeoffs that emerge when an infectious outbreak has established a substantial foothold. The three countries hardest hit by this epidemic lost nearly three full months of national income over the course of only two years. Regional neighbors that were hit in the second round of West African outbreaks were able to intervene when their infection rates were very small, and they did so decisively; they saw both a lower rate of mortality and morbidity and a smaller economic cost. Among the three heavily affected countries, social distancing was unavoidable given the initial scale of the epidemic. But innovations within the health system and in personal protective behaviors played an essential role both in stopping the outbreak and limiting the economic damage it created.
The Facts:
- The 2014-2016 Ebola epidemic in West Africa sickened 28,000 people killing 11,000. The clusters of deaths began in Guinea in late 2013 but were not recognized as Ebola for several months partly because the disease had never been seen so far west in Africa. Ebola had multiple waves as the disease spread to new populations. The rate of new infections seemed to have waned by May 2014. But the outbreak subsequently spread widely through the tri-country region of Liberia, Sierra Leone and Guinea as people who were infected moved across these countries’ porous borders and from rural areas into the capital cities. By the end of June 2014, Médicines Sans Frontières said the Ebola outbreak was “out of control.” The virus then began to appear in a second round of African countries: in Nigeria, when an infected man flew into Lagos in July of 2014, and then later in Mali and Senegal.
- The trajectories of illness and death during an epidemic depend upon the nature of the disease, the government’s policy responses, and the choices people make about their own behavior. Epidemiology models show that, in a worst-case scenario with no policy or behavioral response, an epidemic is contained only as infected individuals become immune or die and the proportion of susceptible people in the population declines. These internal dynamics depend on the contagiousness and virulence of the disease. Ebola is spread through close contact with bodily fluids so it spreads less easily than the novel coronavirus, which is spread through droplets. On the other hand, Ebola is more virulent and deadly than COVID-19 with an average case fatality rate of 50 percent. But public policy and private behavior can also impact the trajectory of the disease. The transmission of an infectious disease is reduced when individuals interact less, or when they interact more safely. Interacting less during an outbreak is referred to as social distancing, and reflects a combination of voluntary choices and official limitations on movement, including quarantines and shelter-at-home directives. Interacting more safely can be achieved through health-system improvements, interpreted broadly to include protective changes in private hygiene practices — such as better hand washing or wearing a face mask when sick to avoid spreading the disease — along with improvements in the diagnosis of infected individuals and their safe isolation and treatment in well-resourced healthcare facilities.
- Health-system improvements are vital throughout an epidemic, first as a complement to distancing in bringing the outbreak under control, and then in allowing a safe return to normal activity. Guinea, Liberia and Sierra Leone faced daunting choices in early August 2014. At the height of the Ebola crisis during late 2014, survey data indicated that roughly half of urban workers employed before the crisis in Liberia were without work, as businesses closed and movement restrictions shut down ordinary life. The best the authorities could do was to select among draconian social distancing policies that created large economic costs in return for crucial but limited traction on the growth rate of infections, and to complement these with massive efforts to improve the health-system response. Policy adjustments reflected ongoing experience, including the failure of coercive official quarantines in the capital city of Liberia and the gradual emergence of evidence on the highly clustered nature of infections. When these countries undertook improvements in the health system, such as the adoption of safe burial practices and the establishment of community care centers, they were able to reduce the rate of transmission much more rapidly than through distancing alone. By early 2015, infection rates had fallen back to pre-emergency levels, and health workers could begin focusing selectively on known chains of transmission. This allowed governments to reduce the intensity of movement restrictions, which they complemented with further health-system improvements. For example, the re-opening of schools during the first half of 2015 was accompanied by a large-scale campaign to improve water and sanitation resources at school sites and train children in proper hygiene. In the final stages of the epidemic, a different but equally important case for health-system intervention emerged, when the public’s perception of a safer environment for interaction encouraged slackening of protective hygiene behavior by individuals, slowing progress against infections and mirroring a behavioral response observed in other epidemics.
- The West Africa Ebola epidemic illustrates the value of preparedness and early policy response in avoiding a lives-versus-livelihoods tradeoff. At the beginning of an outbreak there is a window of opportunity to contain an outbreak rapidly and without major economic cost. This requires that infections be rapidly diagnosed as they occur so the classic strategy of diagnose, isolate, and contact-tracing can be pursued. In recent research, my colleagues and I have compared economic growth in the West African countries that bore the brunt of the 2014 Ebola outbreak – Guinea, Liberia and Sierra Leone – with economic growth in the three “second-round” countries whose first infection occurred either after the WHO’s declaration of a global public health emergency (Mali and Senegal) or very shortly before (Nigeria). In a contrast that was not anticipated at the time, all three of the second-round countries handled their own outbreak with a very small cumulative caseload and minimal economic damage. We estimated that the lack of a policy head start cost Guinea, Liberia and Sierra Leone over 10 percent of annual income per person in 2014-15 — the equivalent of nearly three full months of national income over the course of only two years. By contrast, the trajectories of income per person in the second-round countries were no different from those in the countries of Sub-Saharan Africa that received no infections at all. The most remarkable of the second-round success stories was Nigeria, which used the classic strategy mentioned above to stop an outbreak that originated in Africa’s most populated city, Lagos, two weeks before the WHO declared the global health emergency. The public authorities in Nigeria mobilized immediately, relying on highly experienced local public health experts and taking advantage of a national incident reporting system that had been developed to respond to previous infectious outbreaks. These examples show that having a swift, early response to an outbreak may allow countries to avoid the lives-versus-livelihoods tradeoff altogether.
- Policy responses that scale back an epidemic also reduce its overall economic impact. Social distancing generates a short-run tradeoff that is responsible for the bulk of the economic costs of an infectious outbreak. However, comparing first- and second-round countries, there was no lives-versus-livelihoods tradeoff; instead, countries that acted rapidly enough to contain their outbreaks had better public health outcomes and better economic outcomes. Recent research on the 1918 Spanish flu pandemic appears to be consistent with this point. Western U.S. cities like Seattle and Oakland learned from their predecessors as the outbreak spread west. These cities were quicker to implement official distancing restrictions and to maintain them in place during the fall of 1918. Their outbreaks were contained more successfully, generating fewer deaths and less economic damage than in cities like Philadelphia, which responded with less alacrity and determination. This point has also been emphasized by economists recently in the context of the coronavirus pandemic.
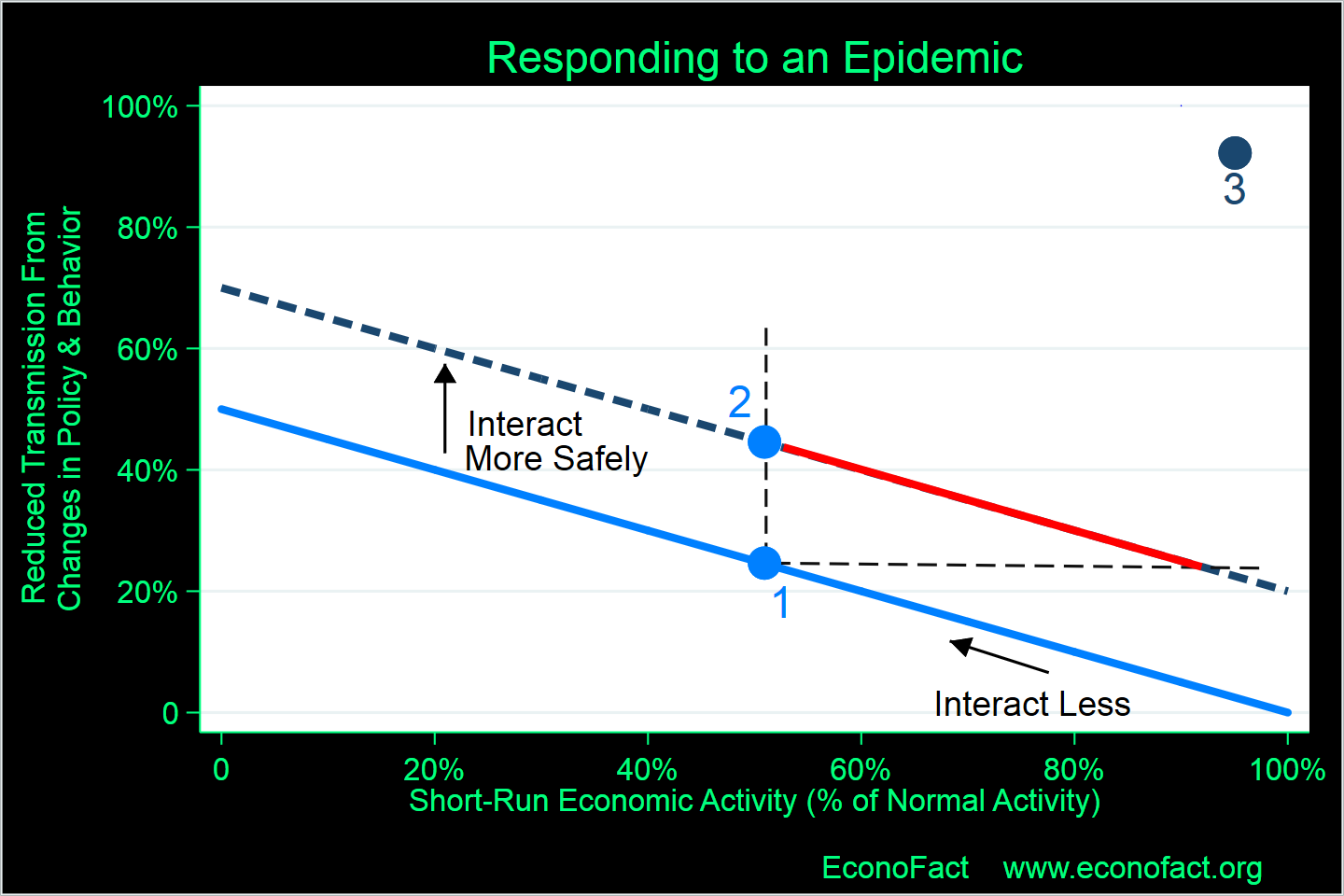
- An analytical diagram can illustrate the policy options and tradeoffs at different stages of an epidemic. Social distancing creates economic losses, because the measures interrupt normal economic activity in stores, factories, offices and schools. The short-run tradeoff associated with social distancing is depicted in the diagram as a downward-sloping line through point 1. An increase in social distancing, as depicted by the arrow, moves the community to the northwest along this line: virus transmission is reduced, as registered by a higher value on the vertical axis, but at the cost of a decline in short-run economic activity, as shown by a lower value on the horizontal axis. At least in the short run, social distancing is subject to a lives-versus-livelihoods tradeoff. But health-system improvements are also vital to containing an outbreak, and they differ sharply from social distancing in imposing little to no cost to the economy. An improvement in the health system may divert resources from other uses, but it is not the key source of economic dislocation during an epidemic. Instead, health-system improvements shift the entire social-distancing line upwards, reducing the infection rate more rapidly for any given amount of social distancing (the move from point 1 to point 2) and even opening up the possibility of distancing more selectively, at a point along the red segment below point 2. For a given state of the health system, the position of the social-distancing line depends on the scale of the epidemic, which shifts the line inwards and forces the community to face a tougher menu of choices in the short run. In the diagram, the second-round countries spent a matter of weeks, rather than months, at a point like 3. In the absence of the policy head start, their infections would have grown to the point where their policy options were no better than those that faced Guinea, Liberia and Sierra Leone, each of which sustained many months of economic damage at points like 1 or 2. The scope for a policy head start of course depends on the context. COVID-19 can be transmitted by individuals who are asymptomatic, by contrast with Ebola which is only transmittable once the individual has become symptomatic. The burden of diagnosis is therefore heavier in the COVID-19 case, because it applies to seemingly-healthy individuals as well as to those presenting symptoms. Seizing the advantage of a head start requires a higher degree of policy leadership in this case: in effect, to impose much more distancing and much wider diagnosis than the observed number of cases (many of which are there but not yet counted) would seem to justify in the eyes of the public.
What this Means:
The distinction between social distancing and health-system improvements has profound implications for public policy during an epidemic. The appropriate tradeoff between social distancing and preserving economic activity depends on the context. Expert consensus favors sharp and protracted distancing restrictions when the epidemic is spreading aggressively, despite the short-run economic costs these entail. These restrictions protect the health system from collapse and overcome the lives-versus-livelihoods tradeoff by limiting the overall scope of the outbreak. The challenging questions then arise about whether and when policy-makers should loosen these restrictions and even pivot towards encouraging economic interaction. Policies to push health-system improvements are crucial in this context because they make room for safe economic interaction. The West African experience shows the importance of early warning systems, preparedness, and continual promotion of appropriate behavioral responses so infections can be diagnosed, distancing can be limited to the known or likely contacts of infected individuals and the rate of new transmissions can be sharply reduced with little economic cost. The importance of health system improvements for slowing virus transmission and mitigating economic damage, both in the midst of an established outbreak and as the pace of new infections begins to slow, cannot be overstated.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.