Severe Maternal Morbidity in the United States
Boston College
The Issue:
The United States (U.S.) continues to be an outlier in maternal health compared to other wealthy nations. Women in the U.S. die from pregnancy and delivery complications at over twice the rate of women in countries such as Canada, Germany, France and Sweden. Rather than improving, maternal mortality has been increasing in the United States since the 1990s and experienced an unprecedented 40% rise during COVID between 2020 and 2021. Moreover, for every maternal death about 60 pregnant women, an estimated 50,000 to 60,000, experience morbidities, which are severe and potentially life-threatening complications during pregnancy and delivery. Consistent with trends in maternal mortality, the rate of severe maternal morbidity has been steadily increasing in recent years. A better understanding of the factors contributing to this rise could help improve women’s health overall and lead to reductions in maternal mortality.
Every year between 50,000 and 60,000 U.S. women experience severe and potentially life-threatening complications during pregnancy and delivery.
The Facts:
- Severe maternal morbidity is defined by the U.S. Centers for Disease Control and Prevention (CDC) as “unexpected outcomes of labor and delivery that result in significant short- or long-term consequences to a woman’s health.” The CDC currently uses a list of 21 diagnoses and procedures to identify delivery hospitalizations with complications, including the need for a blood transfusion, eclampsia, sepsis, hysterectomy, acute heart failure, temporary tracheostomy, and ventilation, among others. Severe maternal morbidity can be a near miss for maternal mortality because without identification and treatment, in some cases, these conditions could lead to maternal death (see here). In addition to these health effects, pregnancies with severe maternal morbidity tend to involve higher costs and longer hospital stays.
- A high proportion of severe maternal morbidities are preventable according to the American College of Obstetricians and Gynecologists. For example, a 2022 review of severe maternal morbidity cases at birthing hospitals in Maryland found that in almost one third of the cases the severe morbidity could have been prevented. Many of those who experienced severe morbidities were high-risk patients that had complications during pregnancy or a history of complications with prior pregnancies, highlighting the importance of identifying and closely monitoring these patients. In addition, 15-20% of the severe maternal morbidity cases in the study involved delayed or no prenatal care.
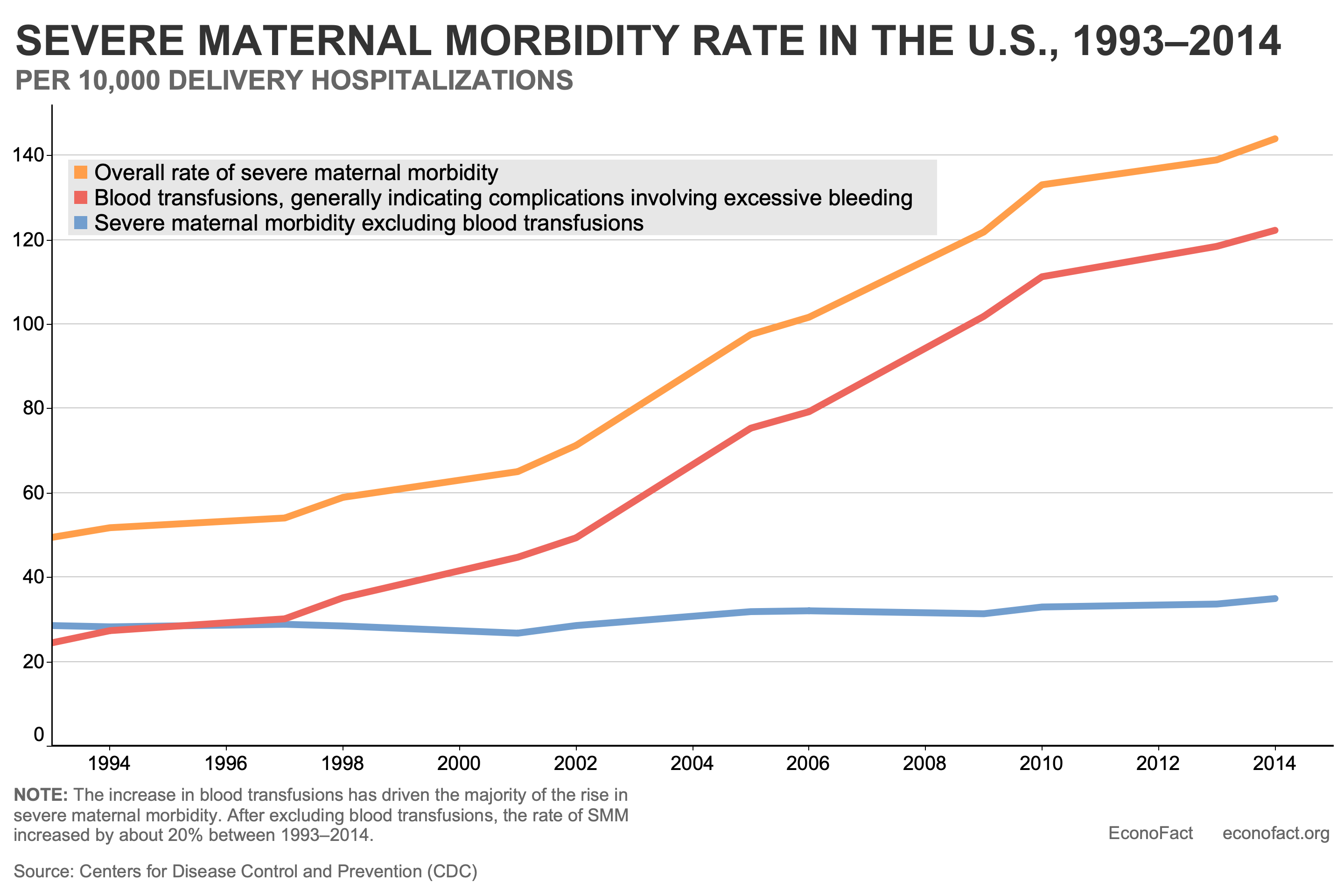
- While only a small proportion of pregnancies in the U.S. experience severe maternal morbidity, the rate has risen steadily since the early 1990s. According to the CDC, 144 out of every 10,000 delivery hospitalizations resulted in severe maternal morbidity in the U.S. in 2014, the most recent year for which national data are available. As severe maternal morbidities are known to be under-reported on the birth certificate and morbidities occur at higher levels postpartum, this is likely an under-estimate of the frequency with which women experience severe complications related to pregnancy and delivery. The rate of severe maternal morbidities in delivery hospitalizations has increased by almost 200% since 1993, largely driven by an increase in the occurrence of blood transfusions — most typically in response to excessive bleeding around delivery (see chart). Hysterectomies (surgical removal of the uterus) and ventilation or temporary tracheotomy (to help patients breathe), are the next most common procedures. They have also risen over time by 55% and 93% respectively between 1993 and 2014 (see here). The reasons for the increase in severe maternal morbidity are not fully understood. According to the CDC, trends that impact the overall health of the population of women giving birth, such as increases in maternal age, pre-pregnancy obesity, pre-existing medical conditions, and cesarean deliveries, could be contributing factors.
- As is the case with maternal mortality, racial and ethnic minority women experience significantly higher rates of severe maternal morbidity relative to white women. Between 2012 and 2015, severe maternal morbidity was significantly higher among deliveries to women from all other racial and ethnic groups compared with deliveries to non-Hispanic white women (see here). Black women experienced the highest incidence for eight of the ten most frequent severe maternal morbidities and were almost twice as likely to experience a severe maternal morbidity than non-Hispanic white women. New evidence indicates that disparities across racial and ethnic groups may be larger than disparities across the income distribution. A recent study that examined birth records from California between 2007-2016 found that Non-Hispanic Black mothers experienced higher severe morbidity rates than non-Hispanic white mothers at all income levels. In fact, the researchers found that infant and maternal health in Black families at the top of the income distribution was markedly worse than that of white families at the bottom of the income distribution in California during the period of the study, suggesting that broader systemic factors may be contributing to these disparities.
- There is an association between state-level changes in reproductive health services and severe maternal morbidity. Over the past decade, social, economic, and political changes have led to legislative and budgetary constraints on women’s reproductive health services. Differences among states in legislative and budgetary actions that impact access to reproductive health services provide an opportunity to test whether these changes are associated with maternal outcomes. In our previous work, we found that a 20% reduction in Planned Parenthood clinics increased the maternal mortality rate by 8% and state-enacted legislation that restricts abortions based on gestational age increased the maternal mortality rate by 38%. In order to examine whether reducing women’s access to family planning and reproductive health services was also associated with rising trends in severe maternal morbidity, we linked state-level reproductive health services data to natality files for 50 states and Washington D.C. between 2009-2018. We found that a 20% reduction in Planned Parenthood centers was associated with a 3.8% increase in 3 delivery-related indicators of severe maternal morbidity: blood transfusion, eclampsia and unplanned hysterectomy. In both of our studies, we found that results were broadly consistent across racial and ethnic groups suggesting that other factors outside the policy arena may be driving these disparities.
What this Means:
Restricting access to reproductive health services is dangerous for women’s health. We found that closing Planned Parenthood health centers increased the risk for pregnancy-related morbidities and mortality, while enacting legislation that limits abortion based on gestational age increased maternal mortality rates. Although the research did not identify the mechanisms, it is possible that clinic closures limit women’s access to or usage of reproductive health services and/or prenatal care that could prevent or mitigate pregnancy-related risks. As access to services becomes more restrictive, it is essential to consider the implications for women’s health. Health centers that provide reproductive health services continue to close, including facilities in rural locations. Since the overturning of Roe v Wade, there is now a patchwork of state access to abortion services based on gestational limits. Eliminating these essential services for many women is putting their health and, ultimately, their lives at risk. It is imperative that policy decisions related to reproductive health services consider the detrimental effects of diminishing access on pregnancy-related morbidities and mortality.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.