Disparities in Access to Health Care During a Pandemic
University of Colorado Denver and Vanderbilt University
The Issue:
The coronavirus crisis has shone a spotlight on existing disparities in access to health care in the United States and on the implications that this uneven access can have in the context of an infectious disease pandemic. Immigrants, especially non-citizens, are less likely to be insured than natives. Moreover, non-citizens are less likely to have a usual place for health care and to cite cost being a barrier to health care. The gap in insurance is driven by differences in access to both public and private health insurance. This gap can lead to worse health among non-citizens, but also, can have negative public health consequences for the general population, particularly in the setting of communicable diseases, such as COVID-19.
Immigrants are less likely to have health insurance than natives. Lack of access to medical care can adversely impact public health in a pandemic.
The Facts:
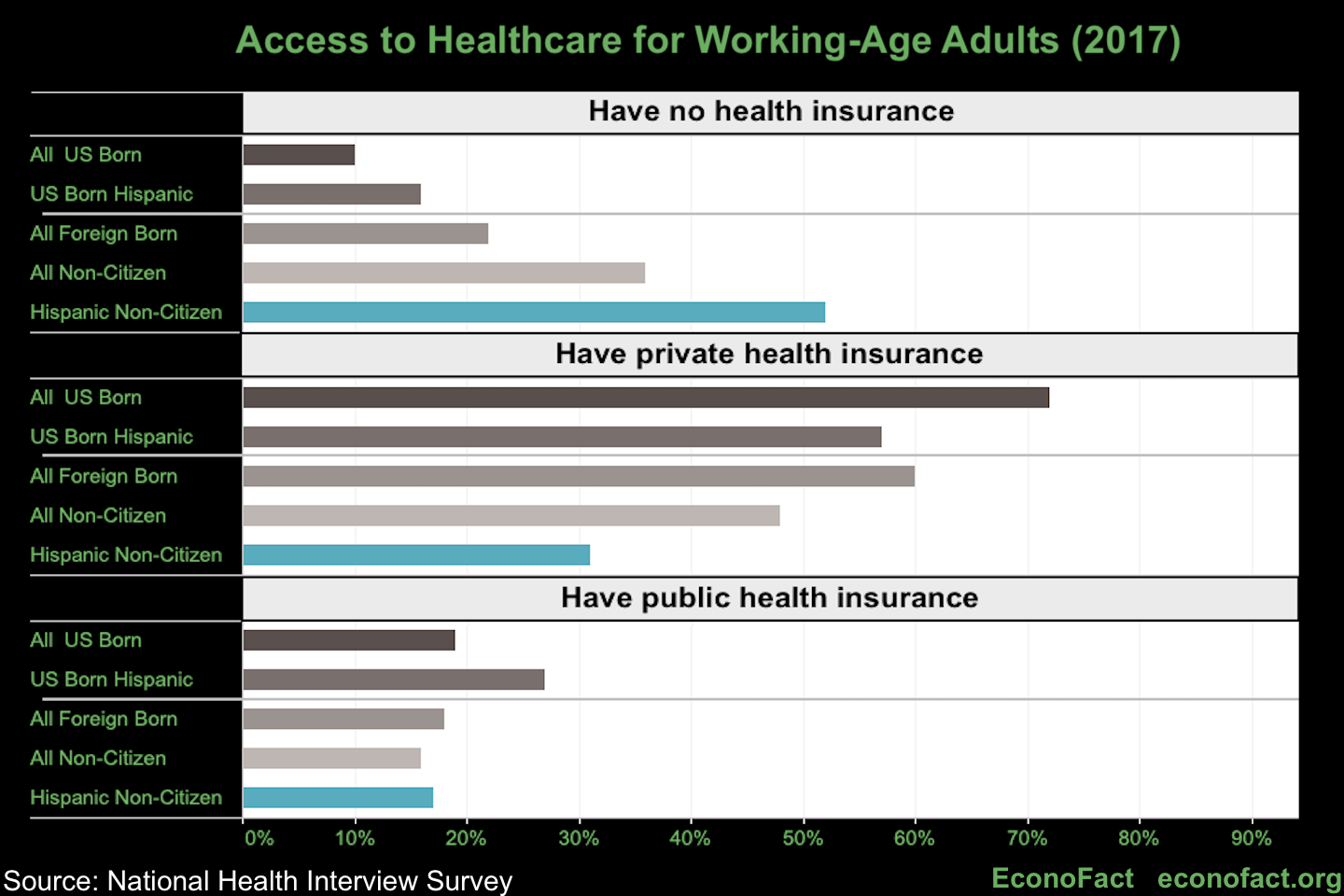
- In 2017, the majority of the U.S. working-age population received coverage through private health insurance (almost 70 percent). An additional roughly 19 percent were covered by Medicaid or other public programs, and 12 percent remained uninsured. However, there are large disparities in access to health insurance between immigrants (foreign-born) and natives (U.S.-born).
- Immigrants, especially those who have not acquired citizenship through naturalization, are less likely to have private health care coverage than those who are native-born. Working-age adult non-citizens are 24 percentage points less likely to have private health insurance than U.S.-born adults (85 percent of all non-citizens are working-age adults.) This gap is slightly wider when comparing Hispanic non-citizens to Hispanic U.S.-born adults (26 percentage points, see chart above). Much of this gap is explained by differences in the availability of employer-provided health insurance. Non-citizens are more likely to work at smaller, non-public firms, which are less likely to provide insurance. Additionally, non-citizens have shorter job tenure and earn lower wages, which limits their access to employer-provided insurance (see here and here).
- Due to limitations on eligibility, Public Health Insurance does not fill in this gap in private insurance coverage; non-citizen adults are 26 percentage points more likely to be uninsured than the U.S.-born adults. The Personal Responsibility and Work Opportunity Reconciliation Act of 1996 introduced new limits on access to Public Health Insurance programs for lawfully present non-citizens. At the federal level, newly-arrived adult permanent residents were made ineligible for Medicaid for their first five years of residence in the U.S. While states could use their own funds to restore eligibility during this period, only eight states did so. Comparing within disadvantaged individuals, who are more likely to meet income eligibility criteria for Public Health Insurance, U.S.-born Hispanics with at most a high school degree are twice as likely to receive Public Health Insurance than non-citizen Hispanics with at most a high school degree (40 percent compared to 19 percent).
- Roughly 40% of non-citizens are undocumented and face greater difficulties in accessing health insurance. However, the gap in insurance between citizens and non-citizens is not solely driven by undocumented individuals: lawfully present immigrants have rates of uninsurance that are double that of citizens. The Kaiser Family Foundation estimates that undocumented immigrants have rates of uninsurance that are four times that of citizens. Undocumented immigrants are ineligible for federal Public Health Insurance programs, except for payment for emergency services (see here). Undocumented immigrants are also more likely to work in low wage jobs compared to lawfully present non-citizens and citizens, which may reduce their access to employer-provided insurance.
- Eligible non-citizen adults have lower participation rates in public health insurance programs compared with eligible citizen adults. This is in part due to fear that receiving public benefits might affect immigration status decisions, which was likely made worse by changes to the Public Charge Rule announced in Fall 2019. With this ruling, the United States Citizenship and Immigration Services (U.S. CIS) expanded the definition of what constitutes "public charge" to include consideration of prior use of food and medical assistance benefits in order to deny immigration to the United States. U.S. CIS has clarified that COVID-19-related health services will not affect immigrants’ status decisions under the public charge rule even if they are paid for by Medicaid. However, immigrant advocates have expressed concern over confusion about the public charge rule reducing COVID-19 testing and treatment among immigrants.
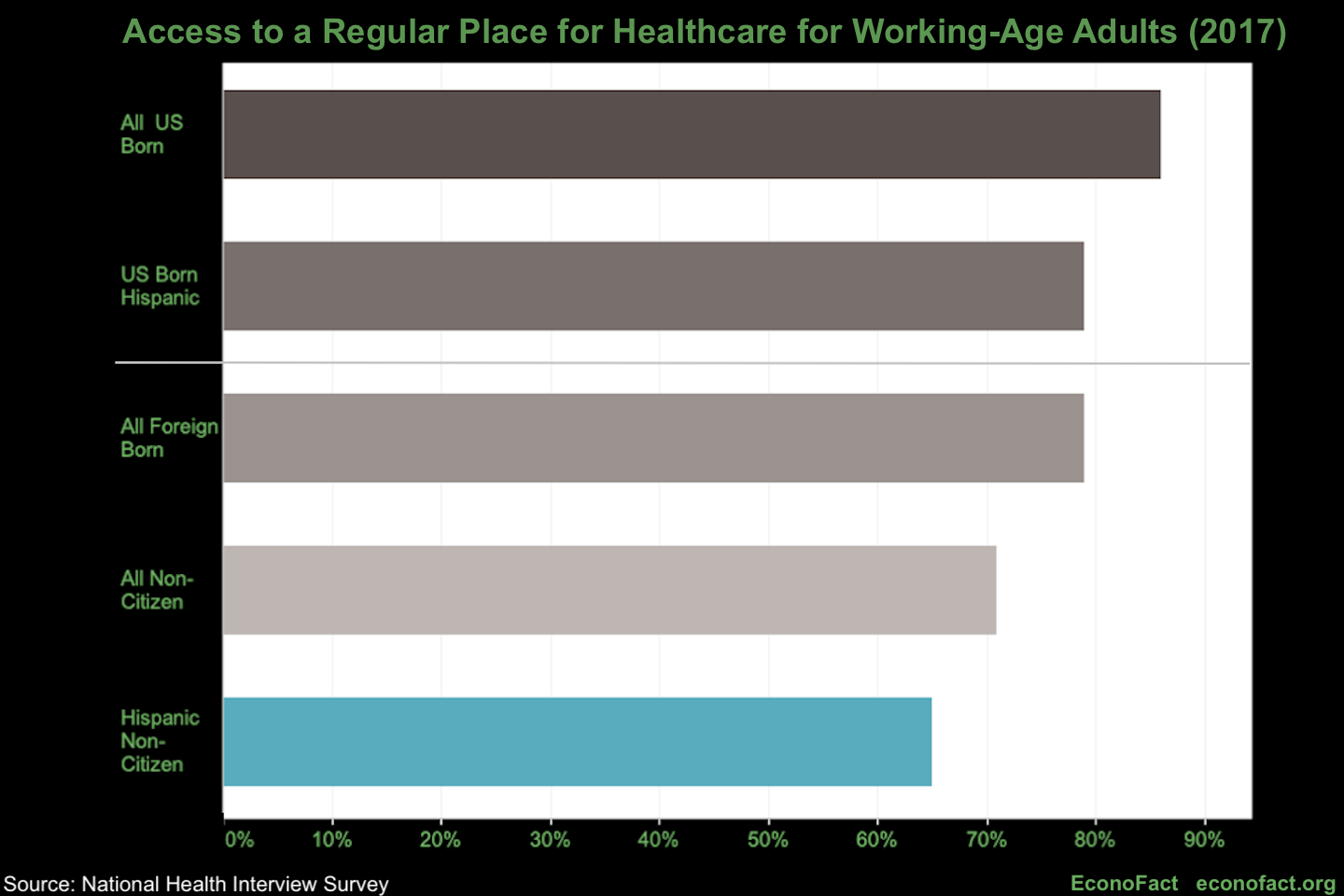
- Non-citizen adults are 15 percentage points less likely than U.S.-born adults to have a usual place to go for health care (see chart below). The most common reason cited for this lack of access to regular health care is concerns about cost. Without access to regular care, non-citizens are likely to have less preventative care, which may lead to costly emergency care in the future. For example, we estimate, with data from the National Health Interview Survey, that only about 29 percent of non-citizens receive the influenza vaccine, compared to 36 percent of U.S.-born adults. Increased vaccination rates would help slow the spread of infectious disease among both the non-citizen and citizen populations.
- In the context of infectious diseases, including COVID-19, reduced access to health care can create a public health risk. Uninsured non-citizens are less likely to have a primary care physician to call in case of symptoms. Large out-of-pocket costs and fear of using public benefits may lead non-citizens to wait to seek care until their symptoms are life-threatening. This avoidance of health care is likely to increase the spread of infection. Borjas (2020) finds that people residing in immigrant neighborhoods in New York City were less likely to be tested, but, among those tested, were more likely to test positive for COVID-19. We find a similar pattern at the national level across counties: a positive correlation between the rate of deaths per person for COVID-19 and the percent of the county population that is foreign-born. While this correlation persists after taking into account urbanicity, number of hospital beds, demographics (age, race, education, and income), and stay-at-home policies, many other factors may contribute to this correlation. For example, Hispanic immigrants may be more likely to work in frontline service jobs requiring face-to-face interaction and a greater risk of infection during the pandemic. At this time, the extent to which lack of health care coverage and fear of interaction with the health care system contributes to this association with COVID-19 severity is unknown.
What this Means:
Non-citizens are less likely to have employer-provided health insurance offered to them through their job. Moreover, limitations on non-citizen’s eligibility for public health insurance, and fear of receiving public benefits, means that non-citizen adults are much less likely to be covered by any health insurance compared to citizens. This also translates into reduced access to health care, including preventative care such as the flu vaccine among non-citizen adults. In the context of infectious disease, barriers to preventive care, testing, and medical attention, can have ripple effects that go beyond the uninsured individuals. People who lack coverage could delay testing or seeking help even when they feel unwell, making it more likely to expose others to contagion in the meantime, which will adversely affect public health. This gap in non-citizens’ access to health care is crucial for policy-makers to consider as the country works to fight the COVID-19 pandemic.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.