Lessons From the 1918 Flu Pandemic
Wellesley College
The Issue:
Much remains unknown and uncertain about the nature of the COVID-19 (coronavirus) pandemic, its trajectory, and the effectiveness of different strategies to slow its progression. While the current situation is in many ways uncharted territory, given the differences specific to the disease and the many changes the world has undergone since the early 20th century, relevant lessons can be drawn from the experience of the 1918 influenza pandemic. The 1918 pandemic, which came to be known as the "Spanish flu" was the most severe pandemic in recent history. While the death toll of the Spanish flu was extensive, it was not uniform. Factors such as the socioeconomic characteristics of the population, underlying environmental quality, and the response by local governments played a significant role in determining how deadly the outbreak was for specific locations and populations.
The death toll of the Spanish flu was not uniform. Socioeconomic factors, pollution, and public action played significant roles in determining how deadly the outbreak was for specific places and populations.
The Facts:
- The impact of the Spanish flu was extensive. One-third of the world’s population is believed to have been infected with the 1918 flu; an estimated 50 million people died, including 675,000 Americans. It occurred in three waves between 1918 and 1919, with the most severe outbreak occurring during the fall of 1918, outside of normal flu season. The 1918 flu affected urban and rural areas throughout the country. World War I likely contributed to the wide dispersion of the flu around the globe. In fact, the disease came to be called the "Spanish Flu" because Spain was a neutral party during the war so its press coverage was not subject to censorship. Although the pandemic likely did not originate in the Iberian Peninsula, it received wide coverage in the press when it arrived in Spain and thus attracted notoriety (see here). The 1918 flu, like the current coronavirus pandemic, was a “novel virus” that had not occurred before. No vaccine was available and treatment options were limited. Efforts to control the 1918 flu were similar to the efforts that we see today: isolation of people who are ill; quarantine of those who have been exposed; and “social distancing” measures such as school closures and public gathering bans (see here).
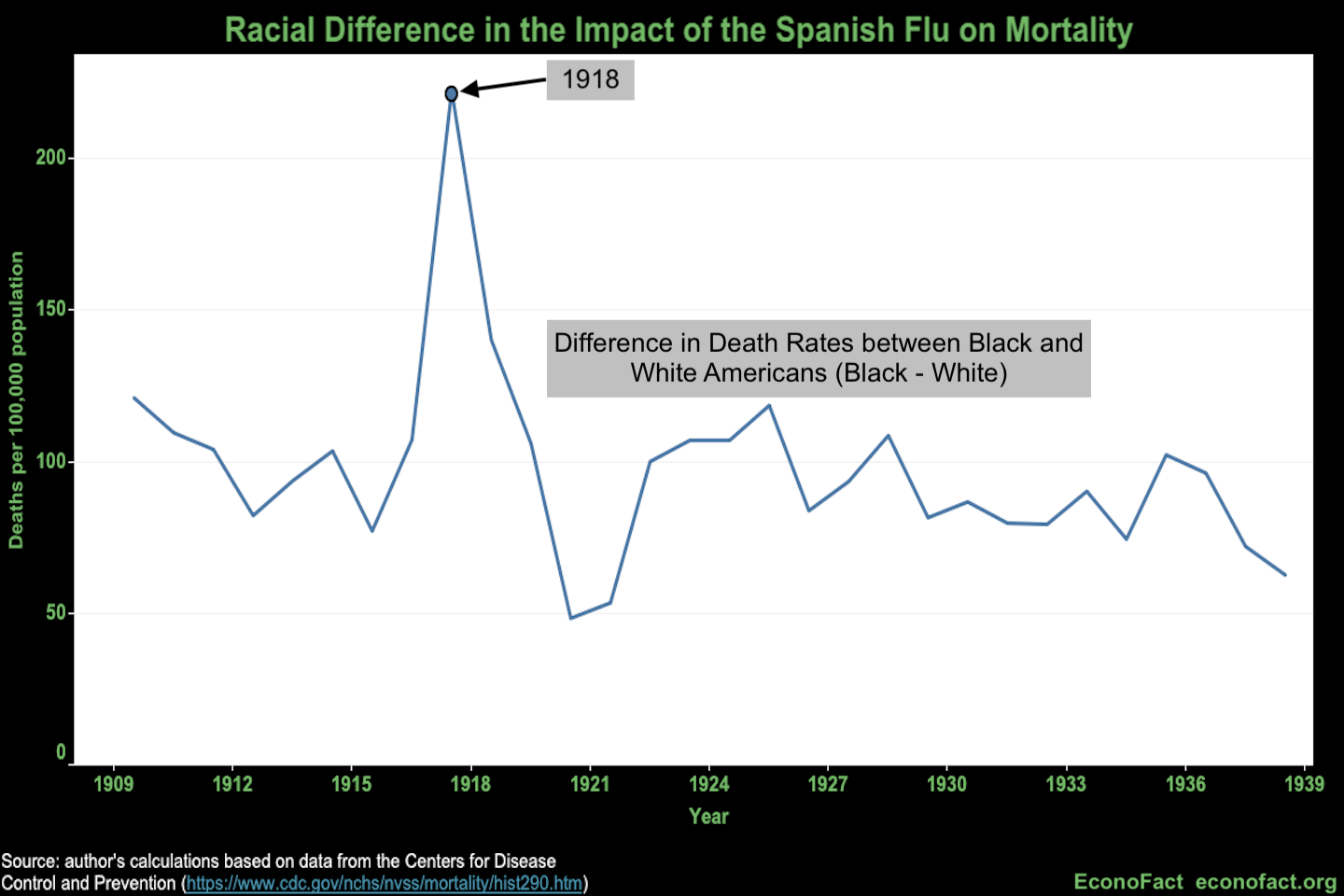
- The impact of the Spanish flu was greater on those with lower socioeconomic status in the United States. We can see that in the differential impact of the flu on blacks versus whites. The increase in mortality due to influenza and pneumonia, the two causes of death associated with the flu, was much larger for blacks than whites during the Spanish flu (see chart). This fact is consistent with a large economics literature showing a strong positive correlation between socioeconomic status and health (see here). In this case, it is plausible that the higher fatality rates for non-whites could be attributable to their lower access to medical care at the time. Or, it could reflect the fact that individuals of lower socioeconomic status lived in closer quarters, which were more conducive to the spread of disease. In addition, it could reflect worse underlying health status or greater susceptibility to the disease. Regardless of the mechanism, this pattern suggests paying particular attention to those of lower socioeconomic status.
- Policies designed to reduce public interactions between people (“social distancing”) reduced mortality. In their research, Howard Markel, Harvey Lipman and J. Alexander Navarro collected and analyzed data on the weekly pattern of deaths in 43 of the largest US cities between September 1918 and February 1919. They augmented these data with the timing and duration of social distance measures, like closing schools and prohibiting large public gatherings. Both earlier enactment and longer duration of such measures were associated with lower overall mortality. They also showed that numerous cities had two peaks in their mortality rates during the fall of 1918, with the first often occurring while social distancing measures were in place and the second occurring after the social distancing measures were relaxed.
- The intensity of the policy response was associated with greater reductions in mortality. We conducted our own calculations using the data from Markel, Lipman and Navarro and extended their analysis, estimating regression models relating these policy interventions to patterns in weekly mortality. Our results indicate that the duration of social distancing measures is the strongest predictor of overall mortality. Every additional day that such measures were in place is associated with reduced influenza-related mortality by 1 death per 100,000 population (or 1,000 people per day at the US population size of around 100 million at the time). We believe that interpreting this result literally may not be warranted, however. A broader interpretation is that a more aggressive policy response reduces mortality; locations that enacted social distancing policies for extended periods also likely did so more stringently. We are not able to distinguish those alternatives given the available data. We also see the utmost importance of “flattening the curve.” Every additional death in the peak week was associated with more than two additional deaths over the entire duration of the epidemic.
- Environmental conditions also affected the severity of the Spanish flu. Recent work by Karen Clay, Joshua Lewis and Edson Severnini shows that poor air quality exacerbated mortality from the 1918 flu. Specifically, they show that cities that used coal in their electricity generation experienced greater mortality from the flu pandemic than cities that relied more on sources that generated less pollution, such as hydroelectricity. If air pollution can generally increase susceptibility to viral infections and heighten the risk of severe complications, post-infection, then this could potentially play a role in the case of COVID-19, too.
- The impact of coronavirus on individual well-being may extend beyond the immediate impact on mortality. The 1918 flu had long-term, intergenerational consequences through its effect on the in utero environment of those who were born in 1919. Douglas Almond compared adult outcomes for the 1919 birth cohort (which was in utero during the flu epidemic) to earlier and later birth cohorts and found evidence suggesting that in utero exposure to the 1918 flu was detrimental to educational attainment and socioeconomic status in adulthood. More recently, Brian Beach, Joseph Ferrie and Martin Saavedra confirmed these findings using alternative approaches, including a comparison of brothers who were and were not born in 1919. Mazumder, Almond, Park and Crimmins demonstrate long-term impacts on health for those who were in utero during the flu pandemic, including higher rates of cardiovascular disease many decades later. The fact that there is evidence to suggest a long-term impact of the 1918 flu does not, of course, imply that there will be comparable effects of COVID-19. It is plausible, though, that the consequences of this pandemic will reach, in some form, well beyond the year 2020.
What this Means:
What can a public health crisis a century ago teach us about our current circumstances? The world is not the same place today, but some of the lessons learned then seem unusually relevant now. What are the lessons? Socioeconomic status matters. Those who have the fewest resources to cope with a public health crisis may be the ones who are most affected. We need to address their needs. The environment matters. Pollution was a contributing factor to mortality 100 years ago. We overlook current environmental issues at our peril. Protecting our children matters. Disadvantages during formative periods of their lives have the potential to have long-lasting implications. Finally, public policy matters. Attacking a public health problem aggressively is important in limiting its damage. We need to take the current coronavirus threat seriously and react forcefully to forestall potentially meaningful loss of life.
Like what you’re reading? Subscribe to EconoFact Premium for exclusive additional content, and invitations to Q&A’s with leading economists.